Adverse childhood experiences (ACEs) are stressful or traumatic events that include a variety of forms of abuse, neglect, violence between parents or caregivers, and other types of serious household dysfunction. Most children face different kinds of abuse, such as physical abuse, sexual abuse, and verbal abuse but few comprehensive studies found adverse childhood experiences in Pakistan. This study examines the relationship between adverse childhood experiences and aggression among university students. Co-relational research design is used through a survey method. The sample includes 400 undergraduates from Rawalpindi and Islamabad universities aged between 18-27 years. The participants were recruited through a convenient sampling technique. The childhood experience Questionnaire (ACE) and Buss-Perry Aggression Questionnaire (BPAQ) were used. Data were analyzed using Statistical Package for Social Sciences. Results suggest a significant positive correlation between adverse childhood experiences and aggression (anger, physical aggression, hostility, verbal aggression) among university students. There is no significant difference between gender and adverse childhood experiences. Moreover, there is a significant difference between gender and aggression. The study offers implications for a university wellness center and therapist working to deal with such students' inability to manage their aggression in the Pakistani context.
Keywords. Adverse childhood experiences, Aggression
In Pakistan, most children face different kinds of abuse, such as physical abuse, sexual abuse, and verbal abuse. Sahil, an NGO working on child protection, reported that almost 2960 cases have been reported in newspapers related to child abuse. 51% of the victims were girls, and 49% of the victims were boys. Cases of abuse were reported from all provinces, federal, Azad Jammu Kashmir, and Gilgit Baltistan. Most of the culprits were acquaintances or parents, service providers (molvi, teachers, shopkeepers, and drivers) (Sahil, 2020). In 2019, 2846 child abuse cases were reported, whereas, in 2020, 2960 child abuse were reported. There is a 4% increase in cases in 2020. This shows that more than 8% of children are abused in Pakistan daily (Hassan Abbas, 2020).
In Pakistan, abuse can occur at every socioeconomic level, ethnic group, religious group, cultural background, and educational level. These abuses can be overcome through awareness, especially in educational settings. In Pakistan, the more vulnerable age to child abuse were the children in the age bracket of 6 to 15 years (Sahil, 2020). Adverse childhood experiences are the events when a child experiences the involves stress or trauma, which include verbal abuse, physical abuse or sexual abuse, neglect given by parents or guardians and any kind of violence between held during childhood, any kind of substance abuse taken by parents (Springer et al., 2003).
According to statistics around the globe, every year, almost one billion children aged between 2-17 years’ experience any form of violence (Hillis, 2016). A survey conducted by the CDC across 25 states of the USA in 2021 reported that 61% of individuals had experienced one type of adverse childhood experience (Centers for Disease Control and Prevention, 2021).
The consequences of adverse childhood experiences were discussed in research conducted in Turkey, which shows childhood maltreatment has many consequences such as short-term well as long-term consequences of adverse childhood experiences at all stages of life, including psychological, economic, and physical effects, with particular emphasis on relationships with mental illness (Yumbula et al., 2010). These experiences play a significant role in shaping their life. Adverse childhood experiences include all types of abuse and neglect, including parental maltreatment, any member's prison, and domestic violence. Also, divorced or mentally ill parents could cause trauma to the child.
Adulthood traits such as difficulty forming relationships, paranoia, insecurity toward others, and introversion can be seen because of unhealthy and/or distant relationships with the family, internalization of this relationship model, and insecure attachment issues in childhood (Renn, 2002). Having actively learned about all of this violence through social interaction, the person may develop an aggressive personality or even start engaging in violent behavior themselves. Aggression and anger are included in the diagnostic criteria for PTSD in the DSM-V manual. It lists "irritable behaviours and angry outbursts" as symptoms of PTSD (Ross, 2015).
Aggression and violence among humans are serious public health issues. Aggression is usually seen to be multi-factored. Genetic variables, the prenatal environment, obstetric problems, the rising environment, biological factors, and mental illnesses such as substance misuse, psychosis, depression, and personality disorders are all predisposing factors for aggression (Citrome & Volavka, 2003).
University students are a good sample for research purposes as they come from different social backgrounds. They are going through changes in their social life as they are more exposed to society (Education Indicators in Focus, 2003). These late adolescents and early adults are fully energetic, active, and enthusiastic (USC Center for Excellence in Teaching, 2003).
In university life, students face many problems due to new environmental settings; many challenges include their career adoptions, relationships, and future goals (Education Indicators in Focus, 2013). These situations in university students make them unique to study on them, as they face different challenges and circumstances due to which they exhibit their behaviours and emotions in this stage of life.
Literature Review
When a child experience maltreatment, it results in stress in his/her early childhood, which increases the risk of stress later in their life. This increases the likelihood of developing psychological problems such as stress, anxiety, and depression. Also, they have a pessimistic view of life which has negative consequences (Bremner, 2003).
Suppose a developing human is repeatedly threatened to stress. They are starting to produce high levels of stress hormones such as cortisol. The human body can learn that this is a typical stress response. Daily life stressors will damage the cardiovascular system and cause different health issues (Whitworth, Williamson, Mangos, & Kelly, 2005).
In another study, researchers found that individuals are not more likely to have secure attachments if he/she exposed to early trauma in their life. In adulthood, they have unresolved attachments with their family, friends, and peer groups (Murphy et al., 2014). Child maltreatment has a significant impact on psychological problems. These factors will influence their social, relationships, emotional, and behavioral problems (Kaplan et al., 1999). Studies show that male and female adolescents have different patterns of adjustment issues (Wolfee et al., 2001)
According to research, adverse childhood experiences are responsible for up to 54 percent of female suicides (Dube et al., 2001). Individuals with adverse childhood experiences were more prone to commit suicide at some point in their lives (Felitti et al., 1998).
Adverse childhood experiences can negatively influence an adult's life, such as education, career, and income status (Marilyn et al., 2017). Children who at some point witnessed any kind of violence were seen as more likely to engage in externalizing behaviours such as physical aggression and disobedience of rules (DeJonghe et al., 2011).
Adverse childhood experiences did not target only one race, class, or area; every child from all races, socioeconomic backgrounds, and geographic areas reported experiencing adversity. The prevalence rate of adverse childhood experiences is high in the lower class (Busby et al., 2011). These adverse childhood experiences make complex issues in an individual that underpins his/her relationship with the rest of the world (Paradis et al., 2010).
Most of the studies on adverse childhood experiences disclosed that the risk of juvenile delinquency increase when the relationship between a child and parents is abusive such as physical or verbal, or when a child faces neglect from his parents (Prather & Golden, 2009).
In 2018 research was conducted on adverse childhood experiences and their effects on chronic disease. Boullier & Blair stated that people with four or more adverse childhood experiences have a high chance of chronic diseases and mental health problems. Chronic heart disease includes cancer, heart disease, and diabetes (Boullier & Blair, 2018).
Natural disasters or accidents and human-caused traumas are the two categories into which psychological traumas fall. Human-made traumatic events can directly affect an individual's beliefs, view of society, and interpersonal relationships. As a result, psychological traumas resulting from human-made events, such as violence and terrorism, are thought to be more difficult and psychologically destructive than traumas resulting from natural events (Hermann, 2016).
Childhood traumas may directly relate to adult mental health problems (Simsek & Evresnel, 2018), such as depression, anxiety, and stress. Adverse childhood experiences are a concept that brings together numerous types of maltreatment that child experience under one umbrella. It allows understanding better complex childhood situations. The long-term consequence of adverse childhood experiences, such as low self-esteem, plays a role in aggressive behaviours (Walker & Bright 2009).
Amygdala is responsible for emotional regulation in the brain. A certain stimulus causes fear which is directly related to the connection between the stimulus and an adverse event (Tabibnia & Radecki, 2018). For example, if a child is exposed to verbal abuse from his father, he later gets frightened when a man yells because he associates it with past experiences in the amygdala. It can be gradually disappeared when the stimulus occurs with a positive event or when a child lives their presence in a safe environment. Also, it can be changed when the child has a strong imagination and can perceive any potential threats based on past fear experiences (Tabibnia&Radecki, 2018). In 2018, Khodasbandeh and his colleagues researched childhood adversity and its risk factors in a forensic setting. He researched 350 men who were accused of physical aggression. They found that adversity in childhood causes risk outcomes related to violence, aggressive behavior, and low self-esteem in adulthood (Khodabandeh et al., 2018).
A study was conducted on rural postpartum women of Pakistan in 2021 on depression and adverse childhood experiences. A longitudinal study was performed from 2014 to 2016 by using random cluster sampling on 889 women. The result showed that more than 50 percent of women reported adverse childhood experiences. Most commonly, these women faced adverse childhood experiences. Mostly these experiences were physical abuse, emotional abuse, and physical neglect (LeMasters et al., 2021)
A study on aggression was conducted by Erturk, Kahya, and Gor in 2020 with childhood emotional maltreatment (CEM) to check the association between them. They found that early childhood schemas and emotional regulation difficulties link childhood emotional maltreatment and adulthood aggression. The study was conducted on a Turkish sample of 291 participants, 204 were females, and 87 were males using convenience sampling (Erturk et al., 2020). In 2021, at Foundation University in Istanbul, a study was conducted in young adulthood on the relationship between variables of childhood trauma and aggression. The study was conducted on 443 participants who were randomly assigned a sample. Females were 332 and males were 111, with the age range of 18-25. Study results showed a significant correlation between these two variables in young adults (Dinç & Küçük 2021).
A cross-sectional study on adverse childhood experiences with functional identity and impulsivity was conducted on adults in Pakistan. Using convenient sampling, two hundred sixty medical students aged 18 and above were taken from medical universities. The result showed that participants who scored high on adverse childhood experiences reported high impulsivity and disrupted functioning (Sheikh et al., 2018).
This research aimed to determine how adverse childhood experiences impact individual behavior, such as aggression in undergraduates (Pakistan). Adversity often leads to aggressive behaviours such as physical aggression, verbal aggression, anger, and hostility, which could greatly impact their interest in their studies, irritability, and self-confidence. Domestic violence and trauma not only occur in childhood and adolescence but future causes aggression in adulthood (Dinc & Kucuk, 2021). According to Intergenerational transmission theory (Besemer, 2011), children are not passive learners but active learners. They used coping and problem-solving methods when they observed any form of violent behavior in the family. They normalize that behavior and learn it. Therefore, the child adopts it as a method of coping. As a result, they can exhibit violent behavior during childhood and later in adulthood.
Present Study
This research explores the relationship between adverse childhood experiences and aggression. As an existing literature review, there are very few published research on adverse childhood experiences in Pakistan. Most research was conducted in western settings. In Pakistan, due to the sensitivity of this topic, the area is under-researched (Bokhari et al., 2016). This present study aimed to investigate the correlation of the above-mentioned variables in the Pakistani context. Further, aggression has dramatically increased over the past few decades, negatively affecting human interactions and relationships (Zinatmotlagh et al., 2013). Adverse childhood experiences could play a role in aggression among undergraduate students. The negative effects of aggressive behavior impact students' social, academic, and personal life (Smith et al., 1998). The study outcome can help the government implement a maltreatment prevention program as baseline information. Also, this study outcome will help parents, teachers, and therapists about adverse childhood experiences and their consequences on university students. The study intends to find out the relationship between adverse childhood experiences and aggression among university students.
Hypotheses
- There is a positive correlation between adverse childhood experiences and aggression (anger, physical aggression, hostility, verbal aggression) among university students.
- Females will report higher adverse childhood experiences than males
Method
Research Design
This study used a correlational research design to determine the relationship between adverse childhood experiences and aggression among university students.
Sample
The sample of the study includes 400 undergraduates. The sample was taken from 3 private and 4 public universities in Rawalpindi and Islamabad. The data was taken from those aged between 18-25 years. Out of 400 undergraduates, 126 students have not reported any adverse childhood experiences. The inclusion criteria for sample selection were age 18yrs or older, currently enrolled in a full‐time undergraduate program and without physical disability. The participants were recruited through a convenient sampling technique.
Instrument
Adverse Childhood Experiences Questionnaire. In 1998, the Adverse Childhood Experience Questionnaire (ACE-Q) was developed by Felitti et al. It is a 10-item measure. It is used to measure childhood trauma. It measures two broad categories abuse and neglect. In abuse, this questionnaire measures physical abuse, psychological abuse, and sexual abuse. In neglect, it measures emotional neglect, physical neglect, and household dysfunction. A dichotomous scale (yes/no) will use to record responses. The scale shows a reliability of 0.6 to 0.8.
Buss-Perry Aggression Questionnaire. Buss-Perry Aggression Questionnaire (BPAQ) was developed by Arnold Herbert Buss and Mark Perry (Buss, A. H., & Perry, M, 1992). The aggression questionnaire consists of 29 items. The aggression scale includes four subscales (Physical aggression, verbal aggression, anger, and hostility). The test-retest reliability of this aggression questionnaire is 0.78.
Procedure
Permission from universities was taken before data collection. Information was provided about the nature of the research. On the consent form, an e-mail ID was provided to them in case of any queries related to the research. Inform consent was given to the participant in the research. Before starting the main study, a pilot study was carried out on at least 50 students. The data collection was done by directly approaching the students and handing them the informed consent and questionnaires, guiding them to fill out questionnaires and giving them 10-20 minutes to fill the questionnaires. After completion of the given questionnaires, collected data were further analyzed for results.
Ethical Considerations
This present study was conducted with the permission of the authority of the Capital University of Science and Technology. Respondents were briefed about the rationale of the study and to make them aware of how their information was further utilized. Scales were used with the permission of the authors. The consent form was taken for participation in the study. Confidentiality was ensured by anonymizing the information obtained from data collection.
Results and Discussion
Statistical Package for Social Sciences (SPSS version 2021) was used for quantitative analysis. Before analysis, data was entered in SPSS. After that data was cleaned. Then data were further analyzed using this software. Missing values on the SPSS sheet were coded as 9 for the demographics and the administered questionnaire.
For the Distribution of data, descriptive statistics were used. Frequency and percentages were calculated for mean, median, mode, standard deviation, skewness and kurtosis were computed for continuous variables. To check normal distribution of data, value of skewness, kurtosis, normality test and histogram was used for normality testing.
To examine the reliabilities of ACE and AQ by calculating Cronbach’s Alpha (α) Inferential Statistics were computed. Pearson Correlation was calculated to see the relationship between the independent variable (adverse childhood experiences) and the outcome variable (aggression). An Independent-Sample t-test was used to examine the gender differences between adverse childhood experiences.
Reliability of Scales and Subscales
Cronbach’s alpha for ACE was 0.70, which is considered moderate to good reliability (Zanotti, Danielle C et al., 2018). The Cronbach’s alpha calculated by the original author was between 0.6 to 0.8. that is comparable to subscales of ACE in this research. Cronbach alpha for BPAQ was 0.85, for subscales anger = 0.57, verbal aggression =.48, hostility = 0.60, physical aggression = 0.70. Cronbach’s alpha found by the original author was 0.72 to 0.80 (Buss & Perry, 1992).
Table 1
Relationship between adverse childhood experiences (ACE) questionnaire and aggression questionnaire (AQ) among university students (N = 274).
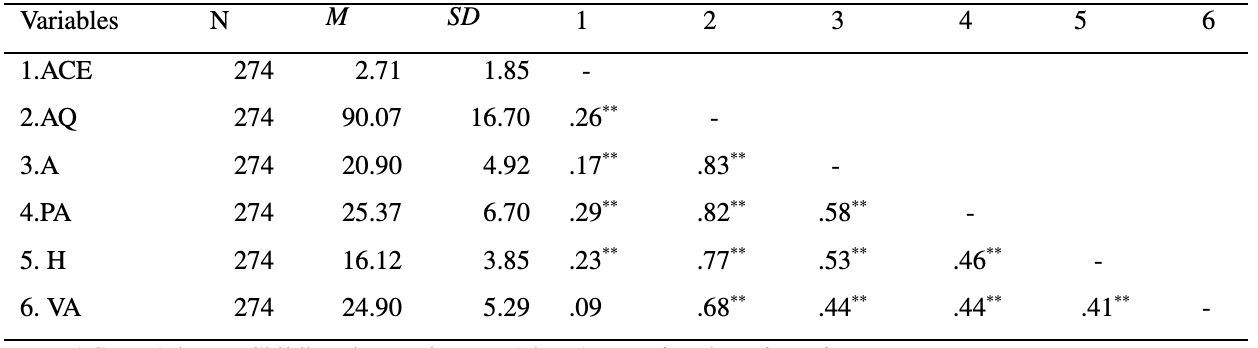
A = Anger, PA = Physical Aggression, H = Hostility and VA = Verbal Aggression. *p < .01
It was hypothesized in this study that there is a correlation between adverse childhood experiences and aggression (anger, physical aggression, hostility, and verbal aggression). Adverse childhood experiences have a relationship with aggression (r= .26, p < .01). Adverse childhood experiences have a relationship with anger (r = .17, p < .01). Adverse childhood experiences have a relationship with physical aggression (r = .29, p < .01). Adverse childhood experiences have a relationship with hostility (r = .23, p < .01). Adverse childhood experiences has a relationship with verbal aggression (r = .09, p < .01). Research determines the significant association between childhood trauma and adult aggression (Chen et al., 2011). Results of the current study show a positive relationship exists between adverse childhood experiences and aggression.
Table 2
Gender differences across undergraduates with adverse childhood experiences scores, aggression (1 or more ACE) and aggression (ACE 0)
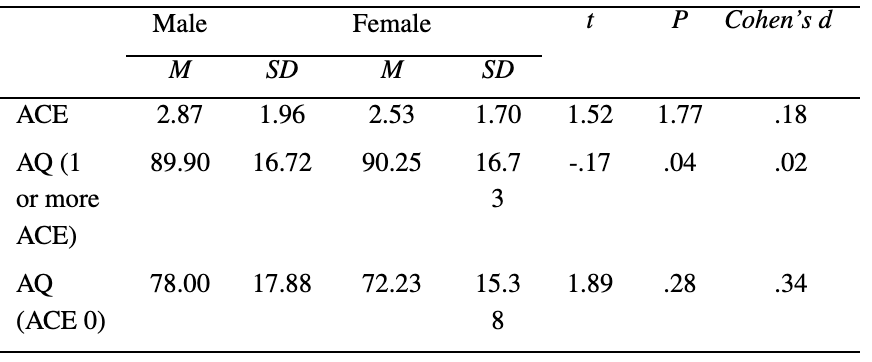
Mean difference was analyzed on adverse childhood experience and aggression based on gender. The result of the t-test showed a non-significant difference exists between adverse childhood, which does not support the hypothesis. In 2016, research was conducted on adverse childhood experiences was conducted in Lahore (Pakistan) to study the relation with impulsivity; their result shows men reported more adverse childhood experiences than females (Bokhari et al., 2016). According to the New York Council on Children and Families (2010), men are significantly more likely than women to have adverse childhood experiences. However, they discovered that women experienced sexual abuse and a household member who was depressed, mentally ill, or suicidal at significantly higher rates than men (New York Council on Children and Families, 2010). Moreover, the t-test shows that female students who experience one or more than one ACE reported more aggression. Also, the present study finds out that students who reported no adverse childhood experiences have no significant gender difference in aggression. These findings would be the cause of social desirability among undergraduates.
Conclusion
This study highlights the gender-specific relationship between adverse childhood experiences and aggression among undergraduate students. It was concluded that a significant positive relationship exists between adverse childhood experiences and aggression among university students. To address ACEs in Pakistan, preventive strategies for gender basis need to be considered. Intervention should be needed for both genders to reduce adverse experiences that begin in childhood and adolescence.
Implications and Recommendations
The present research findings enhance the knowledge that aggression in university students can be due to their adverse childhood experiences. Gender differences in aggression due to adverse childhood experiences are also found. The university wellness center and therapist could use the present research findings to deal with such students' inability to manage their aggression. In Pakistan, preventive programs and campaigns need to be implemented, such as parenting education, early sexual education and mental well-being.
Future exploration may include a community-based approach, in which data may be taken from young adults. Future research should also examine the demographics of socioeconomic status, family system, and class system in relation to childhood experiences and aggression.
References
Awais, S. (2021, August 28). Quality of education in public and private universities in Pakistan Educations.pk https://educations.pk/blog/2 021/08/28/quality-of-education-in-public-and-private-universities-in-Pakistan/
Hassan Abbas (2020, April 22). 2846 child abuse cases reported in 2019: Report. Brecorder. https://www.brecorder.com/news/591347
Boullier, M., & Blair, M. (2018). Adverse childhood experiences. Pediatrics and Child Health, 28(3), 132–137.
Bremner J. D., (2003). Long-term effects of childhood abuse on brain and neurobiology. Child and adolescent psychiatric clinics of North America, 12(2), 271-292. doi.org/10.1016/s1056-4993(02)00098-6
Busby D. M, Walker E. C, Holman TB. (2011). The association of childhood trauma with perceptions of the self and partner in adult romantic relationships. Personal Relationships,18, 547-61.
Buss, Arnold H. and Perry, Mark. P. (1992). The Aggression Questionnaire. Journal of Personality and Social Psychology, 63, 452-459. https://psycnet.apa.org/record/1993-00039-001Centers for Disease Control and Prevention (2021). https://www.cdc.gov/
DeJonghe, E. S., von Eye, A., Bogat, G. A., &Levendosky, A. A. (2011). Does witnessing intimate partner violence contribute to toddlers' internalizing and externalizing behaviours? Applied Developmental Science, 15(3), 129-139.
Dinç, M. E., & Küçük, K. A. (2021). The relationship between childhood trauma and aggression in young adulthood. Health Sciences Quarterly, 5,163-175. doi.org/10.26900/Jsp.5.5.7.
Dube, S. R., et al. (2001). Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: Findings from the adverse childhood experiences study. JAMA, 286, 3089-3096. doi.org/10.1001/jama.286.24.3089
Education Indicators in Focus (2013). How are university students changing? https://www.oecd.org/education/skills- beyond-school/EDIF %202013-N%C2%B015.pdf.
Ertürk, İ. Ş., Kahya, Y., Gör, N., 2020. Childhood emotional maltreatment and aggression: The mediator role of the early maladaptive schema domains and difficulties in emotion regulation, Journal of Aggression, Maltreatment & Trauma, 29(1), 92-110.
Felitti, V.J., Anda, R.F., Nordenberg, D., Williamson, D.F., Spitz, A.M., Edwards, V., Koss, M.P., & Marks, J.S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14, 245-248.
Herman, J. (2016). Travma ve İyileşme, Literatür, İstanbul.
Hillis, S., Mercy, J., Amobi, A., & Kress, H. (2016). The global prevalence of past-year violence against children: a systematic review and minimum estimates.Pediatrics. 137 (3), 2015-4079.
Khodabandeh F, Khalilzadeh M, Hemati Z. (2018). The impact of adverse childhood experiences on adulthood aggression and self-esteem-A study on male forensic clients. Novel Biomed, 6(2), 85-91.
LeMasters, K., Bates, L. M., Chung, E. O., Gallis, J. A., Hagaman, A., Scherer, E., Sikander, S., Staley, B. S., Zalla, L. C., Zivich, P. N., &Maselko, J. (2021). Adverse childhood experiences and depression among women in rural Pakistan. BMC public health, 21(1), 400. doi.org/10.1186/s12889-021-10409-4
M, Sheikh., Sadiq, N., Ahmed., W & Ihtisham, J. (2018). Association of adverse childhood experiences with functional identity and impulsivity among adults: a cross-sectional study. F1000Research. 6, 1978. 10.12688/f1000research.13007.2.
Marilyn Metzler, Melissa T. Merrick, Joanne Klevens, Katie A. Ports, Derek C. (2017). Ford, Adverse childhood experiences and life opportunities: Shifting the narrative, Children Youth Services Review, 72, 141-149.
Murphy, A., Steele, M., RishiDube, S., Bate, J., Bonuck, K., Meissner, P., Goldman, H., & Steele, H. (2014). Adverse childhood experiences (ACEs) questionnaire and Adult Attachment Interview (AAI): Implications for parent-child relationships.Child Abuse & Neglect, 38, 224-233. doi:10.1016/j.chiabu.2013.09.004
Paradis A, Boucher S. (2010). Child maltreatment history and interpersonal problems in an adult couple relationship.Journalof Aggression, Maltreatment & Trauma, 19(2), 138-58.
Prather, W., & Golden, J. A. (2009). Learning and thinking: A behavioral treatise on abuse and antisocial behavior in young criminal offenders. International Journal of Behavioral Consultation and Therapy, 5(1), 75–105. doi.org/10.1037/h0100873.
Renn, P. (2002). The link between childhood trauma and later violent offending: The application of attachment theory in a probation setting, Attachment & Human Development, 4(3), 294 – 317.
Ross, C, A. (2015). Trauma and Aggression in the DSM–5, Journal of Aggression, Maltreatment & Trauma, 24(4), 484-486.
Sahil.(2020). Cruel number 2020.http://sahil.org/cruel-numbers/
Simsek, D., E., & Evrensel, A. (2018). The relationship between childhood traumas and aggression levels in adults.Medicine Science International Medical Journal, 7(3), 1-5.
Slater, A., & Bremner, G. (2003). An introduction to developmental psychology. Blackwell Publishing.
Smith, D.C., Furlong, M., Bates, M. and Laughlin, J.D. (1998). Development of the multidimensional school anger inventory for males. Psychology in the Schools, 35(1), 1-15.
Springer KW, Sheridan J, Kuo D, Carnes M (2003). The Long-term Health Outcomes of Childhood Abuse, J Gen Intern Med. 18(10), 864–70.
Tabibnia, G., &Radecki, D. (2018). Resilience training can change the brain. Consulting Psychology Journal: Practice and Research, 70(1), 59–62. doi.org.ezproxy.loras.edu/10.1037/cpb0000110.
USC Center for Excellence in Teaching (2003). Mentoring university students: Mellon academic mentoring support project. http://cet.usc.edu/resources/teaching_learning/docs/mentorstudents.pdf
Walker, J.S., & Bright, J.A. (2009). False inflated self-esteem and violence: A systematic review and cognitive model. The Journal of Forensic Psychiatry and Psychology, 20, 1−32.
Williamson PM. Kohlhagen JL. Mangos GJ. Whitworth JA. Kelly JJ. (2005). Acute effects of hydrocortisone on plasma nitrate/nitrite activity and forearm vasodilator responsiveness in normal human subjects. Clinical & Experimental Pharmacology & Physiology, 32(3), 162-6.
Wolfe, D. A., Scott, K., Wekerle, C., & Pittman, A.-L. (2001). Child maltreatment: Risk of adjustment problems and dating violence in adolescence. Journal of the American Academy of Child &Adolescent Psychiatry, 40(3), 282–289. doi:10.1097/00004583-200103000-00007.
Yumbula C, Cavusoglua S, Geyimci B. (2010). The effect of childhood trauma on adult attachment styles, infidelity tendency, romantic jealousy and self-esteem. Procedia Social and Behavioral Sciences, 5, 1741–5.
Zanotti, D. C., Kaier, E., Vanasse, R., Davis, J. L., Strunk, K. C., & Cromer, L. D. (2018). An examination of the test-retest reliability of the ACE-SQ in a sample of college athletes. Psychological trauma: theory, research, practice and policy, 10(5), 559–562. https://doi.org/10.1037/tra0000299
Zinatmotlagh, F., Ataee, M., Jalilian, F., Mirzaeialavijeh, M., Aghaei, A. and Shirazi, K. (2013). Predicting aggression among male adolescents: An application of the theory of planned behavior. Health Promotion Perspectives, 3(2), 269-75.

