A Mapping Review and Appraisal of Literature Presenting Clinical Guidelines and Recommendations to Prevent Re-traumatization
ABSTRACT
Rationale: The number of torture survivors is on the rise, posing issues for their care in healthcare settings. Even healthcare experts with training in refugee care are unaware of the health difficulties faced by torture survivors. Any medical evaluation or treatment has the potential to re-traumatize torture survivors, thereby reactivating trauma symptoms without applicable guidelines to prevent re-traumatization. Objective: Our objective was to identify, characterize, evaluate, and organize current, available evidence presenting existing recommendations and suggestions to prevent re-traumatization during the treatment of torture survivors’ physical diseases in healthcare services. Methods: A comprehensive search of electronic databases was conducted. Gray literature coverage was obtained by searching for publications from relevant associations and healthcare organizations focusing on torture survivors. Clinical practice guidelines (CPGs) and research focusing on somatic healthcare services for adult torture survivors, regardless of study design, were eligible for review. Studies that concentrated on psychiatric departments were excluded. To conduct an overview of the available research and describe the scope and distribution of evidence, a mapping review methodology was used. Results: Forty out of 13,111 initial citations met our criteria. There were two guidelines, and text and opinion statements predominated. Two authors independently assessed the risk of bias in each primary research study using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for the research design. Conclusions: This mapping review identifies triggers that may re-traumatize torture survivors during treatment and makes recommendations for prevention. Only a few studies have considered torture survivors’ perspectives on treatment and re-traumatization. According to the findings of the mapping review, healthcare providers should consider survivors’ biopsychosocial situations, demonstrate cultural sensitivity, and change their personal attitudes. They must also identify tortured patients and determine when professional interpreters should be used.
Keywords: Mapping review Torture survivors Re-traumatization Guidelines Recommendations Somatic healthcare services
Introduction worldwide. Torture is defined as follows:
“Any act by which severe pain or suffering, whether physical or mental, is intentionally inflicted on a person for such purposes as obtaining from him or a third person information or a confession, punishing him for an act he or a third person has committed or is suspected of having committed, or intimidating or coercing him or a third person, or for any reason based on discrimination of any kind” (United Nations, 2022, p. 20).
Defining torture is important because perpetrators are often law enforcement officials or members of security services seeking to extract a confession from the victim (Luci, 2017). The involvement of an authority figure in acts of torture is a consequential factor that contributes to the reactivation of
The exact prevalence of torture is unknown, yet a sizable number of asylum seekers and refugees are torture survivors (Ostergaard et al., 2020). The physical and psychological repercussions of torture are significantly unreported (Weisleder and Rublee, 2018); thus, survivors endure complicated physical and mental health difficulties requiring medical treatment (Luci and Di Rado, 2019).
A survivor’s basic trust in others may be destroyed after being subjected to brutal violence inflicted by another person (Bell et al., 2019). Due to people in official positions and healthcare providers being involved in torture (Jones, 2019), survivors’ mistrust of healthcare providers is reinforced. Therefore, every medical assessment or treatment has the potential to reactivate trauma symptoms, and the fear connected with this can lead to re-traumatization (Jacobs and Iacopino, 2001). Healthcare professionals in departments treating physical disorders are frequently unsure of how to identify and interact with traumatized patients; thus, re-traumatization is a risk (Juhler, 2004).
Re-traumatization occurs when memories, feelings, or thoughts of torture trigger the reactivation of trauma symptoms (Duckworth and Follette, 2012). Depending on survivors’ reactions and adaptational styles to past traumatic experiences (Alexander, 2012) and potential triggers, re-traumatization may cause serious and lasting post-traumatic stress disorder (PTSD) symptoms (Schock et al., 2010; Watson, 2016). Thus, healthcare personnel who treat traumatized patients must acknowledge re-traumatization and the nature of traumatic memories, including conscious and unconscious recollections of torture (Schock and Knaevelsrud, 2013). The reactivation of trauma symptoms may occur because of a new traumatic experience or as a result of treatment-related stimuli. Trauma-related stimuli during treatment may include interactions, the environment, medical equipment, and pain associated with medical procedures (Schock and Knaevelsrud, 2013). Patients who experience re-traumatization may experience flashbacks (intrusive memories accompanied by a sense of reliving past events in the present) (Brewin, 2015), nightmares, and other symptoms during or after treatment. Knowledge of potential reactions during re-traumatization as well as the ability to help patients when such reactions occur will improve healthcare professionals’ competency. Identifying stress reactions can help healthcare professionals identify indicators of re-traumatization and initiate adjustments to stop the process as well as help patients cope with treatment-related issues.
Electrocardiograms (ECG), gastroscopy, a general medical examination, or dental treatment can reactivate memories of torture and cause re-traumatization (Gruber and Byrd, 1993; Høyvik et al., 2019). The re-traumatization of torture survivors during treatment is caused by a combination of variables, such as a lack of competence of healthcare personnel and inadequate adjustments of services (Murray and O’Donnell, 2013). In an overloaded workday, healthcare professionals often lack the time or resources to carefully consider the underlying evidence supporting all the decisions they must make. Therefore, medical recommendations are essential for decision-making support (Allodi, 1991).
Understanding how trauma affects patients enables healthcare providers to identify trauma symptoms and respond trauma-informedly, potentially avoiding re-traumatizing patients (Grossman et al., 2021). Furthermore, developing clinical practice guidelines (CPGs) based on existing evidence on torture survivors can improve healthcare quality while driving evidence-based practice (Gerrish et al., 2007). To make informed treatment decisions and identify research needs, evidence about torture survivors’ experiences with both torture and healthcare is required. Nonetheless, there are challenges with recruiting responders as well as ethical concerns (Dickson-Swift et al., 2007); therefore, research on torture survivors is limited (Clark-Kazak, 2017). It is critical to map evidence to determine whether there is sufficient evidence for treating torture survivors, preventing re-traumatization, and identifying research gaps in this area. This process will aid in the selection and prioritization of the research areas.
A comprehensive review of the relevant research in the field is essential before engaging in a meaningful discussion about how to minimize the re-traumatization of torture survivors during treatment in departments treating physical diseases. With our strategy, we aimed to systematically locate literature containing recommendations for treating torture survivors as well as to provide an overview of the literature on healthcare factors serving as triggers for re-traumatization. Furthermore, we planned to identify research gaps and make recommendations to improve research on the treatment of torture survivors in somatic departments as well as to facilitate the prevention of re-traumatization during treatment.
2. Methods
A systematic mapping review (Grant and Booth, 2009) of published literature on the treatment of torture survivors in departments other than psychiatric departments was conducted as part of a larger study aiming to develop and assess the feasibility of a set of clinical guidelines for the prevention of re-traumatization of torture survivors (Schippert et al., 2021). The goal of systematic mapping is to describe the scope of research in a field and to identify gaps in the research base where additional primary research is required as well as areas where no systematic reviews have been conducted (Petersen et al., 2015; Grant and Booth, 2009). Inspired by Katz et al. (2003), six steps were chosen to construct a map of recommendations for the prevention of re-traumatization during treatment of torture survivors in somatic healthcare services: (a) identify the evidence map scope, (b) define key variables, (c) establish a comprehensive search strategy, (d) identify the study’s inclusion and exclusion criteria, (e) systematically retrieve, screen, and classify evidence, and (f) report findings on the map (Katz et al., 2003).
a) Identify the Systematic Map Scope
The initial scope focused on the main recommendations related to (1) identifying torture survivors, (2) preventing re-traumatization, and (3) potential triggers causing re-traumatization. These issues were addressed during a meeting with healthcare providers (general, surgical, and anesthesia nurses working in a surgery department). Several themes manifested as healthcare providers faced challenges when treating torture survivors. Four questions emerged from the themes and were used to ensure a thorough review of the evidence. 1. Is there any evidence regarding the treatment of torture survivors providing recommendations to prevent re-traumatization during treatment in somatic departments? 2. Is there any evidence that certain triggers may cause retraumatization? What triggers are mentioned in the literature? 3. Which recommendations does the research provide for managing triggers to prevent re-traumatization? 4. How strong is the evidence on the treatment of torture survivors in somatic healthcare, presenting recommendations to avoid retraumatization? Text, opinions, systematic reviews, clinical guidelines, questionnaires, case series or reports, and websites were used to answer these questions.
b) Define Key Variables
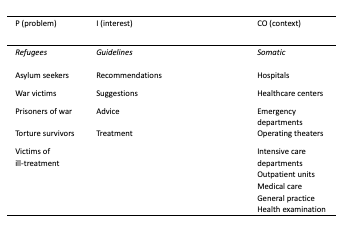
To obtain the targeted and relevant search results, we structured our search strategy using a modified version of the problem-interest-context (PICO) framework (Scells et al., 2017). We searched bibliographic databases using keywords aligned with the PICO elements of the research questions. A combination of medical subject headings and text word terms (Yu, 2018) were employed per the database thesaurus, as shown in Table 1.
c) Establish a Comprehensive Search Strategy
We searched through nine databases and websites as well as reference lists from relevant publications and major article citations. Additionally, we examined gray literature sources for non-indexed guidelines and studies (Paez, 2017). A full description of the search strategy is shown in Table S1, and the sample search conducted on MEDLINE is depicted in Table S2.
d) Identify the Study Inclusion and Exclusion Criteria
The eligibility criteria for the literature to be reviewed included clinical practice guidelines (CPGs) and studies providing recommendations for the treatment of adult torture survivors in somatic healthcare services, independent of study design, published from January 2000 to November 2022. The study contexts were limited to healthcare facilities in somatic healthcare services. Clinical practice guidelines, except those designed only for use in psychiatric treatment, were included. Studies in English, French, Spanish, Portuguese, and Scandinavian languages were considered. The search results (n = 13,111) were uploaded to the Covidence article management system (https://www.covidence.org/), a web-based software program that assists researchers in screening references and extracting data. Following the removal of duplicates, eligible studies were identified by screening titles and abstracts. Then, based on full-text records, potentially relevant studies were screened against the eligibility criteria. Two review authors independently performed title/abstract and full-text screening. Disagreements were resolved through discussion until consensus was reached; a third reviewer was consulted when necessary to reach a consensus. Table S3 displays the inclusion criteria. Fig. 1 presents the flow of reports and studies into the synthesis.
e) Systematically Retrieve, Screen, and Classify the Evidence. This review mapped and organized 40 records by attributes. Table S4 lists the study’s aim, country of origin, study design, publication year, sample size, and context.
f) Report Findings on a Map
Recommendations emerging from the records were extracted and organized in a table. Later, the recommendations were organized by.
the following themes: recommendations to identify torture survivors in healthcare, triggers potentially causing re-traumatization, and recommendations to prevent re-traumatization. This process is illustrated in the results section with the subheading “Themes.” To condense the text in the results section and the tables, all included records were given a number from 1 to 40 as shown in the appendix.
2.1. Quality included records assessment
To assess the methodologically included studies’ limitations, two authors independently assessed the risk of bias for each primary research study using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for the studies’ research design (Briggs, 2017; Jordan et al., 2019; Santos et al., 2018, Briggs), and a risk of bias table for each included study was completed. The quality assessment includes an overall assessment of the finding’s confidence per the Grading of Recommendations Assessment, Development, and Evaluation – Confidence in the Evidence from Reviews of Qualitative Research (GRADE-CERQual) approach (Lewin et al., 2015; Lewin et al., 2018b; Lewin et al., 2018c). The CERQual assessment rates the quality of the findings based on the following characteristics: (1) methodological limitations, (2) relevance to the review question, (3) findings coherence, and (4) data adequacy based on richness and data quantity supporting the findings. Based on the judgments made for the four aforementioned CERQual components, the assessment was divided into four levels: high, moderate, low, or very low (Lewin et al., 2018a). The quality of the included CPG was assessed using the Appraisal of Guidelines Research and Evaluation (AGREE) Instrument, Version II (AGREE II). The procedure has been previously published (Schippert et al., 2021). To ensure a standardized approach, the reviewers (ACS and AKB) completed the AGREE II online training tutorials before conducting the quality assessment (Brouwers et al., 2016). For the CPGs, a quality score was calculated for the AGREE II (described in Fig. S1) six domains using the formula shown in the AGREE II User’s Manual (Brouwers et al., 2010).
3. Results
3.1. Characteristics of the included studies
Nineteen records (47%) were conducted in the United States (US), 10 (25%) in Western Europe, and 6 (15%) in North Europe. Three studies (7.5%) were conducted in Canada, one (2.5%) in New Zealand, and one (2.5%) in Australia. No relevant studies from the African continent or South America were identified. One study was jointly conducted in the United Kingdom and Denmark (31), and another was jointly conducted in the US and Portugal (35). (Study numbers appear in a list in the Appendix.) Although we intended to include literature written in Norwegian, Danish, Swedish, Portuguese, Spanish, French, and German in addition to English, no non-English records met the inclusion criteria for this mapping review. Twenty-three articles comprised text and opinion statements. Two documents from the Center for Victims of Torture in the US (39, 40) focusing on torture survivors in primary healthcare were included in the gray literature search. Two sets of guidelines were included in this review: One from Canada (20) focused on immigrants and refugees in general healthcare and one from England (7) focused on torture survivors receiving healthcare in detention. Furthermore, 35% (k = 14) of the records were published before 2010, and twenty-six (65%) were published between 2010 and 2022. Twenty-three (58%) of the included records were text opinion papers, five (12.5%) were reviews, two (5%) were case reports, four (10%) were qualitative studies, and two (5%) were cross-sectional studies. Studies by context are outlined in Fig. 2, and Table 2 shows an overview of included publications by country and design and included participants by sex and by designation. A description of all included records is illustrated in Table S4




3.1.1. Characteristics of text and opinion statements
Twenty-three (57.5%) records were text and opinion papers. Three (13%) focused on torture-pain treatment (1, 31, 32). These and other studies (35, 36) offer suggestions on how to ask patients about torture and other aspects that healthcare professionals must be aware of and have knowledge about. One record focusing on dental treatment provided suggestions for how healthcare providers should respond when patients reveal traumatic experiences (11). Cultivating trust and safety is mentioned in connection with communication, the use of rs, and disclosure. Cultural competency, sensitivity, and the importance of using a multidisciplinary team to treat torture survivors are also depicted as important (2). One study focusing on skin lesions after torture (6) presented recommendations about physical examination and patients’ need for control (specifically, recommendations on how to ask about torture and mentioned unexplained conditions and the importance of referring survivors to mental healthcare). Asylum medicine and best practices were the focus of one paper, recommending the need to acknowledge scars and acquire knowledge about torture methods (8). Eleven articles focused on the general healthcare context (recommendations about the need for sufficient time when treating torture survivors as well as the importance of having knowledge about torture and being aware of the challenges of being a torture survivor). Suggestions about adjustments to the environment were also presented. Using professional interpreters, the necessity of cultural competence and empathy in treating torture survivors was described in this context. Grodin (2004) and Mollica (2004) provided recommendations for identifying torture survivors (35, 36).
Reports including potential triggers (9, 11, 17, 26, 30, 31, 33, 35, 38) also provided recommendations regarding the use of interpreters, physical examination and control, sufficient time to treat the patient, ensuring patients’ privacy, cultivating relationships of trust and safety, inquiring about torture, healthcare professionals’ awareness of torture, and the utilization of a multidisciplinary team when treating torture survivors. Moreno and Grodin (2002) highlighted the neurological sequels of torture, described triggers inducing re-traumatization, and provided suggestions about communication and the use of interpreters (30). Cultural competency, sensitivity, and awareness were also addressed (30) and echoed in other papers (11, 34). Three articles focused on the importance of trauma-informed care (9, 21, 25); one focused on the connection between low-quality outcomes and discriminatory attitudes among healthcare providers (25) and the importance of promoting staff well-being. When providers can recognize and seek support for their emotional responses to the work, including burnout, compassion fatigue, and secondary trauma reactions, they may contribute to preventing the re-traumatization of patients during treatment (9).
3.1.2. Characteristics of the reviews
Two systematic reviews (3, 27), two literature reviews (12, 37), and a clinical review (28) were included. These focused on the treatment of persistent pain (3), primary healthcare 27), and human rights and medical assessment (37). Suggestions on pain assessment, identification of torture survivors, asking questions about torture, and the importance of referring survivors to mental healthcare were included. Zander et al. (2015) provided an interview guide for use by primary healthcare professionals (27).
3.1.3. Characteristics of the case reports
Two papers with case reports were included. One (14) focused on the surgical treatment of veterans, presenting recommendations about adjusting the environment, preparation before treatment, and considerations about medication and post-anesthesia care. Another study (18) reported treatment with antiretrovirals and medication as potential triggers.
3.1.4. Characteristics of the qualitative studies
Four qualitative studies (5, 10, 15, 23) were included. In one study (23), semi-structured interviews were used to explore neuropsychological assessment and the use of professional interpreters. The findings recommended providing extra time for the medical assessment to cultivate the ability to listen to patients and give them a sense of control. Lønning et al. (2021) interviewed 46 experts and practitioners to explore the challenges and opportunities professionals see and experience in seeking to provide adequate treatment for torture survivors. Suggestions about specialized and interdisciplinary competency were given as one priority to improve the quality of healthcare delivered to torture survivors (15). Board et al. (2021) focused on healthcare services for pain and interviewed 13 participants. Recommendations about how to ask about torture in a clinical context are given (5). One study focuses on dental care by examining interviews with 10 torture survivors and provides recommendations on how to deal with potential triggers during treatment, the use of interpreters, and the importance of improving healthcare professionals’ knowledge about torture (10).
3.1.5. Characteristics of the cross-sectional study
Two cross-sectional studies (13, 29) were included. One study (29), including 121 patients, focused on the identification of torture survivors among a general patient population. This study recommended building trust and asking questions about torture and suggested strategies for effective communication. It also suggested using a multidisciplinary team to treat torture survivors. Kira et al. (2022) focused on the torture effects in the context of Covid-19 and how discrimination as a concurrent stressor with Covid-19 amplified the impact of torture on patients’ symptoms (13).
3.1.6. Characteristics of the websites
Two websites were included. One (40) provides a manual that primary care providers can use to ease the suffering of refugees and help them begin the healing process. This website presents recommendations about using interpreters and the importance of educating patients on how to handle trauma and trauma reactions. The second website (39) aims to help healthcare providers evaluate the current methods used for interviewing, diagnosing, and treatment planning.
3.1.7. Characteristics of the guidelines
Two clinical guidelines were included in this mapping review (7, 20). Pottie et al. (2011) offers evidence-based clinical guidelines for immigrants and refugees. It recommend using professional interpreters at disclosure and increasing cultural competency and sensitivity to improve awareness about issues related to torture survivors. Cohen and Green (2022) list recommendations that aim to increase the identification of torture and healthcare outcomes and to reduce the risk of causing harm during treatment (7). Suggestions on how to facilitate disclosure are given while focusing on using sufficient time, building trust, using interpreters, and providing a suitable quiet environment with privacy. According to Cohen and Green (2022), healthcare professionals must identify and report torture.
A map of the included studies’ characteristics appears in Table 3.
3.1.8. Characteristics of the records presenting triggers
Most records examining triggers are text and opinion papers, followed by qualitative studies, reviews, and websites. Although case reports and cross-sectional studies provide only a few triggers, one qualitative study focusing on dental health present several triggers. Only one guideline offered a few triggers (7). For some triggers, no recommendations for how to manage them were identified.
3.2. Themes
The emerging themes from the included studies were organized, and Fig. 3 shows the conceptual map constructed after the mapping review, including the main recommendations for how to prevent the re- traumatization of torture survivors during treatment.
3.2.1. Recommendations for the identification of torture survivors
Eight records emphasize the importance of knowing the details of a patient’s torture history (3, 6, 26, 27, 28, 31, 32, 37). Trauma, medical, and family histories should be assessed in torture survivors. Regardless of when it happens, torture can affect the clinical picture; and not knowing the patient’s trauma history can lead to major errors in assessment and treatment. Healthcare providers can diagnose, treat, and refer patients better when they know the patient’s history. Studies have suggested asking patients broad questions about their health and life to identify past traumas: Ask whether any circumstances, items, or treatment interactions cause significant feelings or reactions.
3.2.2. Recommendations for preventing Re-traumatization during treatment.
In this category, we included outcomes related to general recommendations, awareness knowledge, building trust, physical examination, interdisciplinary teams, documentation, communication, adjustments during treatment, and using interpreters.
- General Recommendations
Most of the recommendations identified in the records were included in this category, and 20 records are represented (4, 6, 7, 9, 10, 11, 15,16, 20, 21, 22, 24, 25, 28, 29, 30, 31, 37, 39, 40). Some recommendations emerged regarding the need to educate providers regarding the importance of addressing biological, social, and psychological patient needs. Healthcare staff should be educated about torture and its effects (7, 11, 14, 31) to understand what situations, objects, or interaction aspects can cause re-traumatization. This education can facilitate treatment (28, 30, 32) and allow them to adjust, neutralize, remove, or adapt triggers to patients’ needs and special situations (31, 35). To protect patients against re-traumatization, it is recommended that racially and culturally responsive inpatient care (9) and implementation of trauma-informed care (7, 9, 21, 25) emphasize safety, trust, choice, collaboration, and empowerment (7). For clinical interviews, survivors should be assessed individually (34) in comfortable surroundings offering ample time if needed (14, 16, 23, 30). In clinical settings, every refugee patient should be treated as a possible torture survivor. Observe other risks like if patients are members of a minority group, if they were persecuted for political, religious, or for sexual orientation reasons. Torture and related traumas should be deemed as health issues by healthcare providers, and torture should be considered in patients with unexplained psychological, skin, neurological, or orthopedic disorders.
Trauma survivors may experience a transient rise in trauma symptoms after recounting their stories or during some medical procedures. Explaining what to expect during visits is vital. In the initial interview, treatment strategies must be established. Gender concerns are important, especially for sexual assault survivors. The patient may prefer female doctors, especially for gynecology. Some refugees who are persecuted by their own cultural group may prefer healthcare providers from another culture.
Healthcare personnel should not presume that memory in-
consistencies indicate history falsification when assessing torture. It is crucial to understand the histories and discuss them with patients. Patients should be referred to a mental health professional for psychological assessment and therapy when needed.
- Awareness
Recommendations about aspects that healthcare providers must be aware of related to torture survivors’ treatment in somatic healthcare services emerged from 10 records (1, 2, 5, 6, 10, 12, 15, 17, 24, 31).
Healthcare providers should comprehend how a patient’s migratory status affects them as well as how sociocultural issues and difficulties in adjusting to a new culture affect survivors. Due to the involvement of health professionals in torture, survivors may mistrust them. When examining patients, healthcare practitioners must consider the pain-fear dynamic. Understanding how shame and embarrassment can result from exposing torture, especially sexual torture, can help healthcare workers better comprehend patients’ reluctance to reveal their torture histories. When counseling torture survivors, healthcare providers must be conscious of their own subconscious personality traits (5).
- Building Trust
Recommendations on how to create trust and safety were presented in 11 records (2, 6, 7, 16, 17, 19, 24, 28, 31, 34, 37).
It is advised to wait until trust has been established before inquiring about trauma history (37), and torture trauma should never be explored until trust has been established (34). Trauma disclosure can be distressing when made in unsafe circumstances, when patients do not trust healthcare providers, or when made by relatives or children. On the other hand, torture survivors may take a long time to trust others. Survivors





may perceive healthcare professionals as government agents or the healthcare institution as a government institution, making them hesitant to reveal information if they do not understand the confidentiality that characterizes patient-professional relationships (28). Trust is especially important in medical settings because aspects like the use of uniforms (28, 30, 31, 33) can serve as a reminder of healthcare providers’ participation in torture (33). Building trust with survivors may also be facilitated if healthcare providers know the customs of the survivor’s culture (2, 28, 34), use sufficient time to build trust, and engage in compassionate listening (17). Using professional interpreters, allowing extra time for translation, and giving patients control over their treatment may all help build trust (28). Trauma-informed care emphasizes trust and choice (7), allows patients to discuss their individual preferences and needs, and ensures provider-patient confidentiality (also including the interpreter). When interpreters are present, physicians should be aware of potential drawbacks, and when interpreters are fellow nationals, confidentiality issues can arise. Telephone interpreting may be preferred in some cases because it is anonymous, and it is best if the same interpreter is used for all the refugee’s healthcare appointments.
- Physical Examination
Six records presented recommendations related to the torture survivor’s physical examination (6, 7, 8, 17, 19, 30). The patient’s history and physical examination should be consistent. Physical sequelae, such as chronic long-term pain, should not be overlooked. Healthcare providers should try to obtain explanations for scars, which they should measure, describe, and record in text using a diagram. Somatic problems can be exacerbated by new stress, therefore, they should be evaluated as both mental and somatic. Furthermore, the examination room should not resemble a prison cell, should be free of curtains or folding screens, and should be at a comfortable temperature. Healthcare providers should always explain procedures, give patients a sense of control, and allow them the ability to terminate interviews or stop examinations at any time.
- Communication
Four records presented several recommendations related to communication (7, 24, 28, 37). Healthcare providers may observe torture patients’ nonverbal responses to inquiries and treatments to see if the questions are sensitive and if they want to explain or clarify their replies. Providers may also be unfamiliar with refugee communication habits, including avoiding eye contact and shaking hands with the opposite gender. Thus, doctors must comprehend their patients’ cultural backgrounds. Because of the perceived power imbalance in their relationships with healthcare professionals, torture survivors may be hesitant to initiate conversations about torture and other traumatic experiences. As a result, even if they have physical torture evidence, survivors may be hesitant to tell their life stories and share information about traumatic experiences. Full disclosure and assessment of survivors’ healthcare needs demand good communication skills (7).
- Adjustments and Procedures During Treatment
Recommendations related to necessary adjustments and procedures during treatment were presented in 13 records (3, 9, 10, 11, 14, 23, 28, 30, 31, 37, 38, 39, 40).
The records suggest that procedures that are reminiscent of torture, such as those involving electrical equipment or scans performed in enclosed tubes, be thoroughly explained. In most cases, procedures can be completed if healthcare providers do so. To reduce flashbacks, healthcare providers should create a tranquil environment, explain planned procedures, obtain fully informed consent, and facilitate the patient’s control over procedures. Acute care can be difficult for survivors due to a lack of time for psychological preparation. For elective surgical hospitalizations, patients should receive an orientation and even walk through operating rooms and recovery rooms ahead of time. The anesthesia team and nurses should be on the lookout for the emergence of flashbacks. It is recommended that the consistency principle be followed by using the same staff throughout all treatments. Intraoperative sympatholytic therapy as well as patient education on the emergence of flashbacks, agitation, and interventions, may help patients cope with stressful situations during treatment.
Preparations for treatment should include a preoperative assessment consisting of medication control to identify medication used for psychiatric conditions and an evidence-based care plan for patients with flashbacks in the post-anesthesia care unit (PACU).
Patients who meet the criteria for a mental health disorder and require antiretroviral therapy should be offered psychotherapy due to the likelihood of the recurrence of PTSD symptoms. Effective antiretroviral medicines should be offered to torture survivors following exact information and a conversation with patients regarding the medication’s potential role in increasing PTSD symptoms. Providing patients with a sense of control over evaluation methods and listening when they choose to reveal their trauma experiences during treatment is vital. In addition, it is crucial to inform them before making any sudden changes (turning off the lights, touching them from behind, etc.) and to educate them on the importance of taking medications and finishing treatments. Survivors can manage exams and procedures if they are provided with emotional support and information. Some treatments require sedation for evaluation and execution. Providers should discuss incidents of torture with colleagues or seek supervision to preserve a therapeutic mindset and ensure effective treatment. To prevent damaging re- enactments, it is crucial to respond to patients with empathy, detect discrimination, and recognize enactments as well as one’s own attitudes and faults.
- Using Interpreters
In this mapping review, 16 included studies presented recommendations for using interpreters (4, 7, 10, 11, 17, 20, 21, 22, 23, 24, 28, 30, 31, 32, 37, 40).
According to the recommendations, to maximize the quality of clinical encounters and minimize the risks of poor treatment outcomes, bilingual clinicians or certified professional interpreters should be involved in encounters with patients with a torture history. Using professional interpreters is recommended not only to ensure communication with patients but also to give them a sense of control. Interpreters are also covered by the confidentiality principle, and both healthcare providers and interpreters should be careful when dealing with sensitive topics. Tips for working with interpreters include reassuring the patient about confidentiality, maintaining eye contact, speaking directly to the patient, and using short, simple sentences with frequent pauses. The use of relatives as interpreters is not recommended because patients may not fully disclose their trauma for fear of hurting their relatives, or relatives may not provide an accurate translation because they are ashamed of the trauma history. At no time should children be used as interpreters for their parents or other relatives; interpreting services should always be offered. Even when survivors appear to be fluent at the first meeting, they may only be conversant in areas associated with education or work; they may not be fluent in describing emotions. It is recommended to always use professional interpreters, to book an interpreter for the first meeting, and thereafter if required.
3.2.3. Potential triggers and recommendations for managing triggers
Of the 40 records, most described specific triggers as potential inducers of the re-traumatization process. Recommendations to neutralize, remove, or adapt triggers to patients’ needs appear in Table 2. More than 50 factors within the clinical situation are presented as triggers potentially causing re-traumatization during treatment. Negative interactions with healthcare providers due to aggressivity, lack of interest, and lack of empathy are presented as important factors negatively influencing clinical encounters and treatment outcomes (10, 26, 30). According to the recommendations, healthcare providers must show a genuine interest in the patient’s cultural background (4, 24). Most of the records list triggers, but not all offer ways to decrease or prevent re-traumatization. “Healthcare personnel wearing uniforms” is a common listed trigger, but no sources offer advice on how to decrease its impact. Electrical devices, electrodes, and noises are also highlighted, with some suggestions for reducing or eliminating their effects. Fig. 4 shows the 10 triggers that most articles include.
3.3. Quality assessment and evaluation
To assess the methodological limitations of the studies in our sample, we used the JBI Critical Appraisal Checklists. A risk-of-bias table for each included study is presented in Tables S5–S5d. There were minor concerns about coherence related to emerging themes from text and opinion papers and from reviews (i.e., general recommendations, awareness, building trust, how or what to ask, physical examination, communication, using interpreters, treatment, and triggers). The findings are reasonably consistent within and across the included studies. There were no concerns about relevance and there were moderate concerns related to overall methodological quality. Three text and opinion papers raised minor concerns: In Behnia (2004), it was unclear if sources of opinion have standing in the field of expertise; in Nielsen and Jensen (2004), it was unclear if there is reference to the extant literature; and in Willey et al. (2022), it was unclear if any incongruence with literature or sources was logically defended. There were two reviews with minor concerns: In Baird et al. (2017), it was unclear if the likelihood of publication bias was assessed, and in Kassam (2019), it was unclear if methods were used to minimize errors in data extraction.

Fig. 4. The 10 triggers presented by most studies.
The emerging themes from the case reports (i.e., general considerations, treatment, and triggers) were reasonably consistent within and across studies. There were a few concerns about relevance but minor concerns related to overall methodological quality; for example, in Lovestrand & P. Steven Phipps CRNA (2013), it was unclear if the patient’s history was clearly described and presented as a timeline and if adverse events (harms) or unanticipated events were identified and described. Regarding the themes presented in the qualitative studies (i.e., using interpreters and treatment), there were no concerns about relevance and minor concerns related to overall methodological quality (10, 23). The relevance of themes from the cross-sectional studies (i.e., general considerations, identification of torture survivors, what or how to ask, and triggers) were free from concerns, but there were minor concerns with methodology because no confounding factors were identified and no strategies to deal with confounding factors were stated. Concerning themes emerging from the included guidelines (i.e., general considerations, what or how to ask, and using interpreters), there were no concerns about relevance and there were minor concerns about methodology since no confounding factors were identified and no strategies to deal with confounding factors were stated. The CERQual Summary of Qualitative Findings is presented in Table S6.
The total AGREE II score of the two CPGs was, respectively, 264 points (20) and 239 (7) (out of 322), with an overall quality of 80% (7) and 70% (20). The lowest score for 23 individual items was for item 14, “A procedure for updating the guideline is provided” (2 points) for both guidelines. For Pottie et al. (2011), the domain “applicability” had the lowest score (domain 5; 69%); “editorial independence” had the highest score (domain 6; 92%); and domain 4 “clarity of presentation” had the second highest score of 88%. For Cohen and Green (2022), the domain “rigor of development” had the lowest score (domain 3; 56%), while the domains “scope and purpose” and “stakeholder involvement” had the highest scores (domains 1 and 2; 86%). The scores for 23 items by the reviewer and by domain are demonstrated in Table S7.
4. Discussion
To the best of our knowledge, this mapping review is the first to provide an overview of evidence related to torture survivors’ treatment in somatic departments, presenting potential triggers causing re- traumatization and identifying recommendations to prevent re- traumatization. We excluded research within the psychiatric treatment of torture survivors and used an approach that included studies with different designs, reviews, and two CPGs. Psychiatry health personnel are more knowledgeable about trauma effects and are focused on treating trauma, whereas somatic healthcare services aim to treat physical illness by protecting patients from harm interfering with psychological trauma. Accordingly, this mapping review does not include guidelines that only apply to psychiatric departments. Although healthcare professionals working in somatic departments must understand torture trauma and its consequences, they are not intended to treat trauma. Offering recommendations designed only for psychiatry may cause frustration to healthcare providers because of their inapplicability in somatic clinical medical contexts, reducing the possibility of successfully implementing the recommendations (McArthur et al., 2021).
We found evidence related to somatic healthcare services, including physical, sociological, and psychological torture aspects, health, and disease. Our results suggest more evidence of torture survivors’ experiences in healthcare is needed. The results indicate a low proportion of experimental studies involving refugees; most records were text and opinion publications based on the experiences of specialists working with torture survivors and only two studies offered case study research. Case study research is appropriate when the context is pertinent to the phenomenon being studied (Schoch, 2020). As the clinical context is significant to the phenomena of re-traumatization (Schock and Knaevelsrud, 2013), providing case study research of torture survivors’ experiences of re-traumatization during treatment could offer us vital information on the subject. For example, an older case report (Gruber and Byrd, 1993) describes a 42-year-old Vietnamese prisoner of war requiring an endoscopic assessment of the gastrointestinal system. Through descriptions of the healthcare environment, recommendations for healthcare providers to enhance awareness of the special requirements of this patient population to prevent re-traumatization are provided. Our mapping review indicates an underutilization of the case study design for this patient group, which should be taken into consideration when planning future research.
With a comprehensive search strategy, this mapping review includes an important portion of publications within healthcare for torture survivors. The Istanbul Protocol (IP) (Manual on the Effective Investigation and Documentation of Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment) was published in 1999 as a set of common, international guidelines for the assessment of persons who allege torture and ill-treatment. The IP represents an important milestone of bringing a new and bigger focus on torture survivors into healthcare. For example, in 2009, the Forum for Medicine and Human Rights at the Medical Faculty at the University of Erlangen-Nuremburg provided the first German edition of this manual (Furtmayr and Frewer, 2010). By including guidelines and recommendations from the last 20 years, we believe that this mapping review covers new and relevant evidence within the torture survivor’s treatment in medical contexts. Since new evidence typically prompts updating guidelines and recommendations between 2 and 5 years after publication, we may also have covered guidelines published before 1999 and updated after the IP publication.
As the purpose of this mapping review is to summarize and discuss research on advice to prevent re-traumatization of torture survivors, we strive to convey the discovered recommendations in a transparent manner and the overall assessment of confidence in the research findings. Even so, it is crucial to note that some of the offered potential triggers in the included records are based on the authors’ decision to interpret very literally the claims in some retrieved publications that provided little underpinning evidence. Some of the potential triggers were presented in a detailed way and the recommendations for managing these triggers were not adapted to a specific clinical context and may be difficult to apply in everyday clinical settings. The suggestions presented must be interpreted and adapted to the contexts of health professionals. For example, the suggestion of not having curtains is related to issues of avoiding a dark room; nonetheless, the absence of curtains can cause situations where patients become exposed, especially if there are other patients around. These instances requires health professionals to make a concrete assessment of recommendations and adapt them to each situation. Some recommendations may have a background not only in torture exposure but also in cultural aspects. For example, “Touching the foot is the only allowable type of tactile stimuli to reduce fear eliciting risks in touching the upper body” (Lovestrand and Steven Phipps, 2013). These instances may be applicable for some patients, but not all, depending on cultural aspects (Schirmer et al., 2022) and must also be considered in terms of context. If the upper body parts are assessed clinically, this proposal cannot be used. Such challenges may indicate that there is a need to develop applicable recommendations for specific clinical contexts.
Most of the publications represent studies conducted in the US and Western Europe. This effect may be related to the organizational system in these countries where treating torture survivors is delegated to specialized centers, also producing necessary research (Moa Nyamwathi Lønning, 2020). According to Moa Nyamwathi Lønning (2020), Denmark and England are countries in which these types of institutions provide a more structured healthcare response to torture survivors (Moa Nyamwathi Lønning, 2020) and both countries are represented the most in this mapping review’s evidence. Only two records contained clinical guidelines. Although the guidelines are of high quality, the scarce amount indicates a general lack of clinical guidelines for healthcare providers on this topic.
Six studies focused on pain, while some of the other contexts as communication using interpreters, human rights, obstetrics, etc. are only addressed in one publication each. This can be explained by the existence of repetitive research on some themes, as reported by P´erez-Sales et al. (2017), who concluded that recent literature on torture neurobiology and re-traumatization has been among the most innovative and influential (P´erez-Sales et al., 2017). Nevertheless, we could not find publications on re-traumatization related to torture neurobiology. This may be because most of the publications included in this mapping review were text papers from experts and, according to P´erez-Sales et al. (2017), experts may see torture neurobiology as being unrelated to their everyday concerns (P´erez-Sales et al., 2017).
Few studies included participants; only three studies used qualitative interviews. This small number indicates that torture survivors are underrepresented in studies about treatment in somatic departments and re-traumatization. This may also indicate difficulties in recruiting refugees and torture survivors for research. Many torture survivors move around, between and within countries, searching for safety, work, and educational opportunities, indicating that researchers may exert greater effort to include survivors in research (Gabriel et al., 2017) so that their voices also become represented in studies focusing on re-traumatization during treatment in somatic healthcare departments. Furthermore, problems with sampling may create significant biases in the results presented in evidence about our understanding of torture survivors. Such a challenge has been discussed by Gabriel et al. (2017) and Dehghan and Wilson (2019), who provided advice on how to recruit refugees for research studies; ethical considerations related to recruiting torture survivors have also been presented in other publications (Gabriel et al., 2017; Dehghan and Wilson, 2019). A greater focus on this topic may also be needed, supporting research on torture survivors’ treatment in somatic departments (Higson-Smith and Bro, 2010), and efforts to increase the amount of evidence based on torture survivors’ experiences may be a priority.
Participants across the included studies were seldom identified by sex, which can introduce bias into research about torture because men and women react differently to trauma and re-traumatization (Pabilonia et al., 2010). Still, most participants in the studies who reported sex were female. This variance seems to differ from what is presented in the literature as it is more difficult to recruit female participants in a research study on sensitive topics (Gabriel et al., 2017). Some studies included participants under the designation of migrants without specifying how many refugees and how many have experienced torture. Such a lack of specification can constitute bias since there is a difference in the experiences participants carry with them and how they react to trauma and re-traumatization (Holtz, 1998). Tortured refugees may have a different sensitivity level and different pattern reactions from others who have not been subjected to torture (Holtz, 1998; Jaranson et al., 2004).
The main themes from this mapping review provide a better understanding of what is recommended in the literature to prevent re- traumatization of patients with a torture history during their treatment in somatic healthcare services. The themes “Identification of torture survivors,” “Triggers,” and “Recommendations to prevent re- traumatization” provide an overview of the main triggers and recommendations presented in the literature. Identification of patients who are torture survivors is the crucial first step in such a patient’s somatic treatment (Eisenman et al., 2000), requiring healthcare providers to have special skills, such as the ability to suspect and recognize torture survivors and ask them appropriate questions (Eisenman et al., 2000; Clarysse et al., 2019). According to the evidence from this review, healthcare providers’ successful identification of patients who are torture survivors enables them to prepare for patients’ treatment and to prevent re-traumatization. Preparing the environment, searching for information about the patient, the patient’s country, and culture, and removing or adjusting eventual triggers according to the patient’s needs are important tasks for preventing patients’ re-traumatization under care (Johnson, 2005; Moreno and Grodin, 2002; Williams and Hughes, 2020).
Managing triggers is a vital aspect of preventing torture survivors’ re- traumatization during treatment and almost all included studies discuss potential triggers and communicate suggestions for their effective management. It is important to note that some records describing triggers (Milosevic et al., 2012; Johnson, 2005) did not present a solution or intervention for removing or adapting the triggers to patients and situations. These solutions were found in other studies (Moreno and Grodin, 2002; Veliu and Leathem, 2017) or were not directly found in the literature included in this review (Crosby, 2013) and require the readers’ interpretation. This mapping review may contribute to overcoming such a challenge since we tried to organize data. Although some articles had a rich description of triggers and patients’ reactions to them (Høyvik and Woldstad, 2022), there is still a lack of suggestions on how to help patients when re-traumatization occurs, which should be prioritized in future research.
Evidence reinforces the importance of using interpreters even when patients appear fluent due to the difficulties of talking about traumatic experiences (Williams and Hughes, 2020). Additionally, it is recommended to be attentive to the potential secondary effects of using interpreters (Moreno and Grodin, 2002). Thus, healthcare providers must constantly weigh the advantages and disadvantages of using interpreters when treating torture survivors. Further research giving torture survivors opportunities to express their thoughts on this subject is needed.
Providing quality healthcare to torture survivors begins with awareness of a patient’s torture history (Ahrenholz et al., 2015; Mollica, 2004). Knowing the history aids disclosure, facilitates appropriate management of eventual challenges under treatment (Williams and Hughes, 2020), and prevents re-traumatization (Moreno and Grodin, 2002). The subject of asking about torture is described as an inherent tension in the included studies. On the one hand, healthcare providers should ask patients directly about their torture history (Williams and Hughes, 2020) and support them in disclosing it (Mollica, 2004). Healthcare providers, on the other hand, are advised to avoid asking their patients about their torture history due to the risk of re-traumatization (Pottie et al., 2011; Quiroga and Jaranson, 2005). One study proposed that building trust in the medical context could help resolve this conflict (Behnia, 2004). According to some studies, disclosure should be avoided in situations of distrust (Behnia, 2004; Eisenman et al., 2000; Pottie et al., 2011).
Confidentiality related to patient-professional relationships is also mentioned as important to prevent re-traumatization. This concerns the healthcare providers’ ethical obligations to maintain patient confidentiality in treatment settings. The challenge is that this is not absolute, varying within cultures and countries (Jones and McCullough, 2013), causing feelings of insecurity in torture survivors, especially those who experienced healthcare providers’ involvement in torture (Ahrenholz et al., 2015). Torture survivors may also be accustomed to the maintenance of confidentiality in psychiatric contexts, with other possibilities of privacy during treatment and time expended on treatment. In contrast, the context in a somatic medical setting characterized by patients sharing rooms, healthcare professionals rushing around, and the involvement of several healthcare providers in the treatment may be challenging for patients. This demands that healthcare providers adjust and improve the patient’s confidentiality. Although the included studies mentioned the importance of maintaining confidentiality during treatment (Crosby, 2013), specific recommendations to handle described challenges are lacking in the literature. It also applies to the recommendation about employing consistency principles by using the same staff throughout all treatments. Characteristics of the medical context with staff rotation do not allow the use of the same staff through all treatments, but some adjustments can be made. Recommendations including this aspect are also lacking in the included studies.
In our review, two included CPGs provide recommendations concerning “the identification of torture survivors,” “using interpreters,” “physical examination,” “communication,” “general recommendations,” and present “triggers.” In Pottie et al. (2022), we identified the CPG domain “applicability” (how well healthcare providers are able to implement the CPG recommendations in their daily clinical practice) as the domain with the lowest score. In Cohen and Green (2022), the domain “rigor of development” (the process used to gather and synthesize evidence) was the domain with the lowest score. Other systematic reviews of CPGs on other healthcare topics have also presented low scores in these domains (Alonso-Coello et al., 2010). Nevertheless, in the included guidelines in this review, domain scores are above 50% (69% and 56%), causing moderate concerns about the presented recommendations. In terms of assessing the risk of bias, the included studies were found to be trustworthy. Nevertheless, recommendations presented by the included records can be difficult to implement in practice due to a lack of details and advice on how to implement them. Recent records, including one of the guidelines, recommend the implementation of trauma-informed care principles. This shows that literature with a focus on refugees follows the development of such a concept. Still, the included records do not present steps for implementation. This echoes findings in a systematic review reporting that, although the term is widely used, it is not well understood how to apply the concept in daily clinical practice (Raja et al., 2015). Considering the benefits (promoting physical and psychological safety for patients and building trusting relationships with them) that implementation of trauma-informed care principles can bring to the quality of services (Miller et al., 2019), further efforts should be made to develop concrete proposals on how to implement these principles within the treatment of torture survivors in somatic clinical contexts.
5. Strengths and limitations
Our mapping review is the first attempt to synthesize literature presenting recommendations to prevent re-traumatization of torture survivors receiving healthcare treatment, utilizing the JBI Critical Appraisal Checklist and AGREE II to evaluate the quality of the included studies and clinical practice guidelines. Nevertheless, evidence mapping has several limits, so it must be viewed with caution. The limited number of included guidelines was the primary constraint of the study. Despite our extensive systematic search, it is possible that unpublished or non-indexed studies were excluded. We only included records published after 2000; consequently, there may be substantial literature from prior years that were omitted. Another limitation is related to the exclusion of literature referring to psychiatric healthcare services. Including this type of literature in the mapping may have resulted in a richer outcome. Nonetheless, we followed a systematic and transparent review methodology to ensure the identification of the best available evidence. As a result, studies from diverse geographic regions around the world focusing on torture survivors were included. Nevertheless, as only Western nations are represented in the included studies, this may be a limitation of this mapping assessment as well as the difficulty of generalizing the conclusions to non-Western nations. While we hoped to include literature written in several languages in addition to English, no non-English-language publications met the inclusion criteria for this mapping review. As the search emphasized English-only terms, the results of the literature search may have been biased toward English- speaking nations. Most studies were text and opinion papers, and while these were prepared by experts in the field, the survivors’ voices were not as well represented. More research into the perspectives and experiences of torture survivors who are re-traumatized during treatment is needed in the future to better understand this group of patients. More studies presenting healthcare perspectives and difficulties in delivering non-re-traumatizing healthcare services to torture survivors are also needed to supplement the suggestions presented in this mapping review. This viewpoint should be considered when developing future guidelines.
The guidelines included in this mapping review were assessed with AGREE II. We did not have many results from assessments with the same instrument for comparison because there were only two guidelines with similar scores. Overall, the domain reliability rates of AGREE II were high. Nevertheless, AGREE II does not provide an exact cutoff between high-quality and low-quality CPGs, forcing reviewers to decide on the cutoff and adding a source of bias.
The included studies present a few recommendations on how to handle situations in which the torture history is inconsistent with clinical findings or when patients are reluctant to tell their histories, causing healthcare providers to doubt patients. This recommendation refers to how healthcare providers generally meet torture survivors, and as a critical aspect of the clinical context, proposals must address the subject thoroughly. As a result, recommendations on how to deal with inconsistencies in the information provided by torture survivors may be a priority in developing guidelines. Our review summarizes proposals for the prevention of re-traumatization, but we still lack suggestions on how to help patients when re-traumatization occurs. This topic should be worked on and prioritized in further research by offering recommendations on how to detect re-traumatization occurrence during treatment and how to help patients. Parallel to this motion and considering the presented challenges related to torture survivors’ reduced trust in healthcare providers together with challenges related to losing control during the treatment, more suggestions on how to take care of their special needs during perioperative care with general anesthesia are needed.
Future study is required to contextualize the guidance given in the literature to prevent the re-traumatization of torture survivors in healthcare settings.
6. Conclusions
According to the mapping review’s findings, few studies have included torture survivors’ perspectives on their re-traumatization experiences during treatment. Future research should consider this gap, and case studies with torture survivors and other qualitative studies can help build a body of evidence to inform practice. A lack of guidelines on the subject is also a source of concern. Themes emerging from the mapping review suggest that healthcare providers should be aware of survivors’ language support needs, consider survivors’ biopsychosocial contexts, demonstrate cultural sensitivity, and modify their own attitudes. Furthermore, they must identify tortured patients and determine when professional interpreters should be used. Several aspects should be addressed during treatment to manage triggers in a clinical setting, and several potential triggers were presented in this mapping review. Although the review’s goal is to map and present evidence, we included additional information specific to the triggers presented. If these triggers arise in routine clinical practice, we propose avoiding potential triggers.
Appendix B. Supplementary data
as much as possible when no solutions are available and adapting the guidelines to the specific clinical context. This tentative suggestion is a limitation of the mapping review as well as an area for future investigation. Creating context-specific recommendations should be a major priority. More research is also needed to develop more responsive guidelines due to the scarcity of studies and guidelines on the subject. It is critical to include torture survivors in research and to allow them to disclose their re-traumatization experiences during treatment. There are still no recommendations on how to identify symptoms that indicate the occurrence of re-traumatization. Identification of symptoms is beyond the scope of this review, and additional research is required.
6.1. Health administrators must facilitate training for healthcare professionals to
Increase their understanding of torture and its consequences as well as their cultural competency and sensitivity. Health administrators may also prioritize the provision of qualified interpreters. Furthermore, health educators must play critical roles in developing future healthcare personnel’s cultural competence and sensitivity. Healthcare providers should have access to guidelines and standards for treating torture survivors.
Funding
ACS is funded by a PhD fellowship from the Institute of Nursing and Health Promotion, Oslo Metropolitan University, Norway, and Akershus University Hospital (Ahus), Norway.The Norwegian Nursing Association (NSF) provided financial assistance to the study.
Data availability
No data was used for the research described in the article.
a Institute of Nursing and Health Promotion, Oslo Metropolitan University, Oslo, Norway b Akershus University Hospital, Oslo, Norway c Institute of Physiotherapy, Oslo Metropolitan University, Oslo, Norway d Institute of Clinical Medicine, Campus Ahus, University of Oslo, Norway e Norwegian University of Science and Technology: Gjøvik, NO, Norway f Oslo University Hospital, Oslo, Norway g Norwegian Faculty of Medicine and Health Sciences, Gjøvik, NO, Norway
