Conflicted Related Sexual Violence (CRSV) includes all forms of sexual violence where state or non-state armed groups target political, ethnic, or religious minority groups during state collapse. It is highly prevalent in the Democratic Republic of Congo (DRC) and leads to the development of many psychological problems. The present study was based on a Cross-Sectional research design in which data was collected from 52 female survivors of Conflict-Related Sexual Violence between the age range of 20 to 61 years (M = 35 SD = 9.7) in the Democratic Republic of Congo during the period from June 2019 to February 2020.

All participants were assessed through Posttraumatic Stress Disorder Checklist (PCL) (Weathers et al. 1993), the Posttraumatic Growth Inventory (PTGI; Tedeschi & Calhoun, 1996, Brief Cope (Carver, 1997, Life-Orientation Test-Revised LOT-R; Scheier et al., 1994), and Multidimensional scale of perceived Social Support (MSPSS; Zimet et al., 1988). Results showed that there was a significant negative correlation between post-traumatic growth with post-traumatic stress disorder and pessimism; a significant positive correlation with emotion-focused coping and optimism. At the same time, the relationship between post-traumatic growth with age, social support and problem-focused coping was non-significant. Additionally, the result of the hierarchal regression model showed that post-traumatic stress disorder, pessimism, optimism and motion-focused coping play an important role in predicting post-traumatic growth, with pessimism being the most significant predictor. This study highlighted that being optimistic and having a positive life approach play a significant role in the development of post-traumatic growth among survivors of Conflict-Related Sexual Violence.
Keywords. Post-traumatic growth, pessimism, optimism, coping strategies, post-traumatic stress, conflict-related sexual violence
Despite having the world's largest resources and many inimitable features, the Democratic Republic of Congo (DRC) has remained a fragile country for many years. It has struggled with wars, civil strife, d multiple rebellions since 1996 and slowly recuperating from political and economic instability. It has enormous challenges in terms of security/peace, decentralization, political/economic governance, and poverty. Despite some improvement in recent years, females are the most underprivileged part of this country, facing huge physical, mental, and psychosocial burdens. Sexual violence, specifically conflicted related sexual violence (CRSV), is the most threatening traumatic event that is highly prevalent in the Democratic Republic of Congo (DRC). Especially women and children are mostly a victim of it. Every second woman there had encountered rape and sexual violence at some level. It has devastating effects on survivors' psychosocial well-being and mental health (Linden, 2011; Scott et al., 2017). Their psychological pain is clearly depicted by the statement of the UN secretary general's special representative on sexual violence, which was referred to as the rape capital of the world. Sexual violence was used as a weapon of war in this country, and it has one of the world's highest rates of sexual violence. Sexual violence, which may include kidnap, sexual slavery, sexual exploitation, and human trafficking – was a prominent feature of this conflict (Delic et al., 2017), whereby women are believed to have been targeted by civilians, locally-stationed military forces, foreign military forces and United Nations Peacekeepers (Jennings et al., 2009). Previous research revealed that survivors of CRSV develop the symptoms of depression, post-traumatic stress disorder (PTSD), anxiety, and suicidality (Johnson et al., 2010). This is because of the social stigmatization and rejection at the family and societal levels (Kelly et al., 2012). Further, the results of a study on 51 female survivors of sexual violence after 20 years of war in BIH depicted the long-term effects of conflict-related sexual violence. 57% of these survivors suffered from post-traumatic stress disorder (PTSD), 76% reported disrupted sleep, and 40% expressed frequent thoughts about death and dying (Mittelmark et al., 2017). In addition to these symptoms, some other most prominent and persistent emotional and psychological reactions of these victims are often intense fears of associated situations, generalized anxiety, humiliation, depression, increased substance abuse, loss of self-esteem, distrust of others, social isolation, hostility, fear of sexually transmitted diseases, guilt, self-blame and fear of sex or other sexual dysfunctions (Steketee & Foa, 1987; Ullman & Najdowski, 2010).
But these survivors do not always report the negative effects of these experiences. Rather they appear to be strong enough to take these events in an optimistic way and experience positive psychosocial outcomes in the form of PTG (Anderson et al., 2019). Post-traumatic growth is the art of living optimally despite having traumatic events in life. It brings permanent changes in the survivors' lives' psychological, cognitive, and spiritual aspects. Though the process of its development is initiated immediately after the experience of trauma, the actual growth occurs after some time of trauma experience when survivors start reflecting on their trauma at a cognitive level and giving meaning to his/her experience. However, it was highlighted in the literature that both positive (PTG) and negative outcomes (PTSD) of any trauma could emerge at the same time as a separate entity (Solomon & Dekel, 2007); and there is several psychosocial factors which involved in the development of PTSD and PTG among survivors of traumatic events. A study on Bosnian refugees who settled in the USA revealed that coping plays a very significant role; for example, avoidance coping strategies are associated with greater distress and negative outcomes compared to healthy coping strategies (Ai et al., 2003; Lazarus, 1993). Optimistically inclined people can derive a sense of benefit from adversity to a greater extent than pessimistic people, and that optimism can be generalized and remain stable over time (Prati & Pietrantoni, 2009; Saboonchi et al., 2016). So these emotional, social and spiritual resources act as buffers in managing trauma. But there are limited studies that focus on growth following interpersonal events such as CRSV. There is one such study in which a sample of 104women survivors of CRSV from Bosnia and Herzegovina was studied to determine the relationship between post-traumatic growth with symptoms of post-traumatic stress disorder (PTSD), coping (COPE), and optimism. And it was found that coping strategies play a significant role in the development of PTG.
As deliberated above, the female strata of Congo are mostly affected by CRSV, leading to the development of several mental health consequences that need to be addressed for these women's overall well-being. In this milieu, the present study was designed to determine the various psychosocial predictors, such as PTSD, age, gender, coping, locus of control, and social support, which are helpful for the growth of PTG among these survivors.
Method
Sample
The present research was a cross-sectional study in which a purposive sample of 52 female survivors of conflict-related sexual violence was collected from the Democratic Republic of Congo. The sample obtained comprised females with an age range between 20 to 61 years (M = 35 SD = 9.7). Further, details about sample characteristics are explained below in Table 1.
Table 1
Demographic characteristics of the sample (N=52)
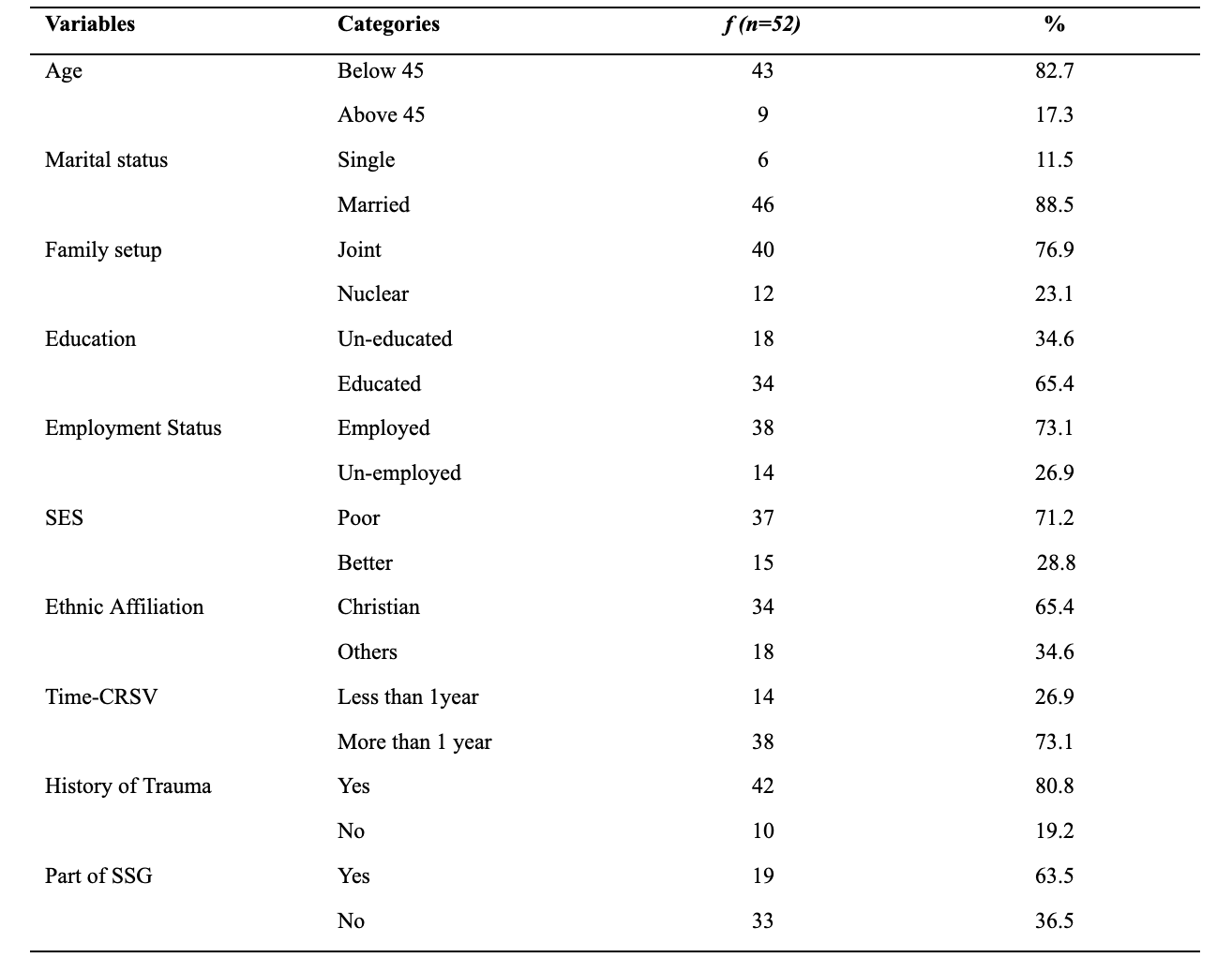
Table 1 shows that all the participants were females (N = 52). Majority of them were married (n = 46), educated (n = 34), employed (n = 38) and living in joint family system (n = 40). Maximum participants were Christians (n = 34) and belonged to poor socio-economic status (n = 37).
Instruments
The following instruments were used to measure the various study variables.
Posttraumatic Stress Disorder Checklist (PCL; Weathers et al., 1993). It is a 17-item self-report checklist of PTSD symptoms based closely on the DSM-IV criteria. Respondents rate each item from 1 = "not at all" to 5 = "extremely" to indicate the degree to which they have been bothered by that symptom over the past month. Thus, the total possible scores range from 17 to 85. Estimates of internal consistency (Cronbach's alpha) range from .94 to .97(Weathers et al., 1993). Test-retest reliability has been reported as .96 at 2-3 days and .88 at one week (Ruggiero et al., 2003).
Post-traumatic Growth Inventory (PTGI; Tedeschi & Calhoun, 1996). The PTGI is a 21-item self-report scale for assessing psychological growth following a traumatic event; in this case, framed in the context of participants' experiences of CRSV. The PTGI includes five subscales: new possibilities, relating to others, personal strength, spiritual change, and appreciation for life. Items range from 1= "I did not experience this change as a result of my crisis" to 6 = "I experienced this change to a very great degree as a result of my crisis," and total scores on the PTGI range from 1 to 126, with higher scores reflecting greater perceived growth. It is a reliable instrument with Cronbach's alpha for the PTGI total score was .96 and ranged from .66 to .90 for subscale scores.
Brief COPE Scale (Carver, 1997). The Brief COPE (Carver, 1997) is a self-report questionnaire used to assess several different coping behaviors and thoughts a person may have in response to a specific situation. The Brief COPE was developed based on concepts of coping from Lazarus and Folkman (1984). The scale comprises of 28 items and fourteen subscales: Active coping (items 2 and 7), use of instrumental support (items 10 and 23) planning (items 14 and 25) was classified as problem-based coping. Self-distraction (items 1 and 19), denial (items 3 and 8), substance use (items 4 and 11), use of emotional support (items 5 and 15), behavioral disengagement (items 6 and16), venting (items 9 and 21), positive reframing (items 12 and 17), humor (items 18 and 28), acceptance (items 20 and 2), religion (items 22 and 27), self-blame (items 13 and 26) falls into emotion-based coping (Macdonald, 2011). Internal reliabilities for the 14 subscales range from .57- .90 (Carver, 1997), and reliability for each subscale ranged from .75 to .82 (Jacobson, 2005). It is a Likert-type scale with responses varying from 1 = 'I have not been doing this at all to 4 = = 'I have been doing this a lot.
Life-Orientation Test-Revised (LOT-R; Scheier et al., 1994). The LOT-R is a 10-item self-report measure of dispositional optimism and pessimism. Three items in the scale capture optimism (Cronbach's α = .70), three capture pessimism (Cronbach's α = .74) and the four remaining items are fillers and are not scored. Scores were calculated in their original unidimensional format. Respondents rate each item on a scale from 0 "strongly disagree" to 4 "strongly agree." A total score is calculated by adding the inverted pessimism score to the optimism score. Cronbach's α for the total score is .73 for the Serbian population (Jovanović & Gavrilov-Jerković, 2013; Scheier et al., 1994).
Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988). This scale is used to measure participants' perception of support that they get from family, friends, and significant others. It is a 12- item self-report questionnaire with a 7-point Likert scale where 1 denotes very strongly disagree and 7 denotes very strongly agree. It contains three subscales, and each contains 4 items. The total mean score can be generated by adding the score of all 12 items and dividing it by 12. A mean score of 1 - 2.9 means low support, 3 - 5 means moderate support and 5.1 - 7 is considered high support. In the present study, MSPSS showed good reliability with Cronbach's alpha of .94.
Procedure
Multi-level procedural steps were carried out in this study; the researcher got formal permission for the use of scale through email and approval from the Ethical committee of the Psychological Research Wing, GHQ. Participants with a history of CRSV from various Villages in Congo were approached. A short-info care session was given to all the participants with the aim of explaining the purpose of the study and obtaining their verbal consent. Data was collected through a language translator.
Results
The collected data was entered on SPSS-24 and analyzed. Descriptive Statistics were carried out to describe the mean, SD, frequencies, and reliability coefficients. Further inferential statistics involved Pearson Correlation, regression analysis, and t-test.
Psychometric Properties of scales
The reliability of all the scales used in this study was tested using coefficient alpha reliability, and it was found that all the scales were reliable, which is shown in Table 2.
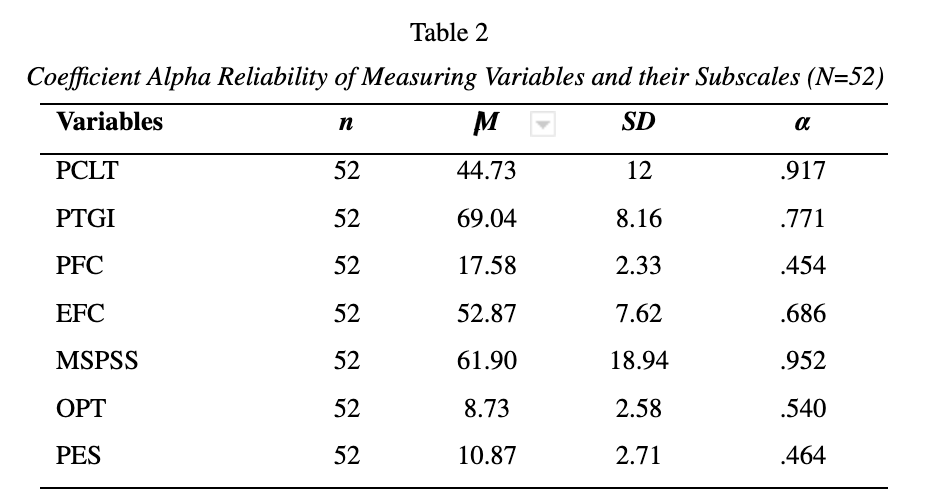
Results show that the value of alpha of all scales ranges from .917 to .454; all represented good values of reliability except two sub-Scales (PFC of Brief COPE and PES of LOT-R) which have satisfactory reliability. This indicates that the data collected in this study has produced reliable results (Heiman, 2011) and could be used for further analysis. The reliability of subscales of the LOT-R was low. The reason behind it is that this scale was composed of 10 items; among them, three items in the scale capture optimism, three capture pessimism, and the four remaining items are fillers and are not scored. As the length of the scale is related to the reliability of the scale, so less number of items might affect the reliability. Another possible reason was the lack of cross-cultural validity of these measures.
Table 3
Frequencies and Percentages of Main Variables (PTSD & PTG) Among CRSV Survivors (N=52)
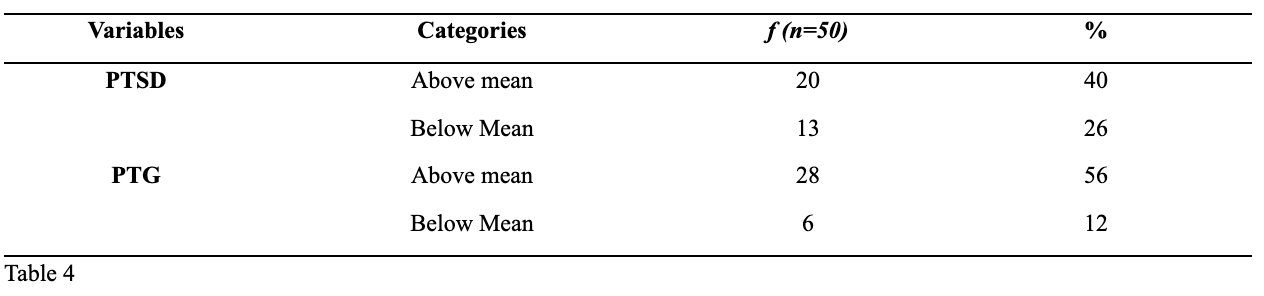
Table 4
Correlation Coefficients of PTG with PTSD, Problem Focused Coping, Emotion Focused Coping, Social Support, Optimism, Pessimism and Age Among Survivors of Conflict-Related Sexual Violence (N=52)
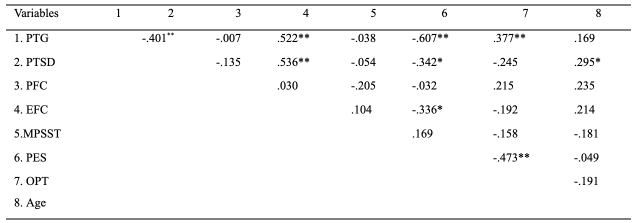
PES= Pessimism; and OPT = Optimism. **p < .01; *p < .05.
Table 4 shows the Correlation Coefficients of PTG with Various study variables. Results revealed that PTG was significantly negatively correlated with PTSD and PES, meaning that survivors of CRSV who have PTSD and Pessimism tend to have poor PTG. Whereas it was significantly positively correlated with EFC and OPT to indicate that survivors who used emotionally focused coping and were optimistic would have high PTG. Further to this, no significant results were reported with other variables such as age, social support and problem-focused coping.) was non-significant.
Regression Analysis
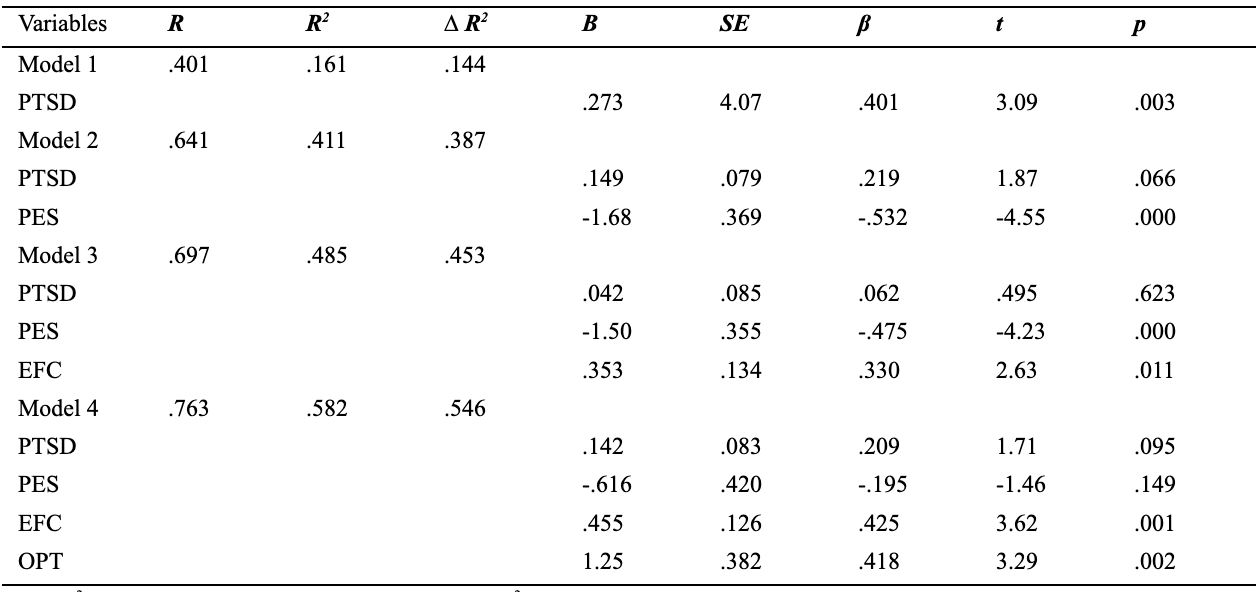
In order to test the hypothesis that PTSD, PES, EFC and OPT will predict PTG among survivors of CRSV, Hierarchical multiple regression was calculated.
The results showed that post-traumatic stress disorder accounted for about 16% (F (1, 50) = 9.59; p< 0.05). In step 2, pessimism was added to the model and the total variance explained by the model was 41% (F (2, 49) = 17.09; p< 0.001), explaining that an additional 25% change is caused by pessimism. In the nest model, emotion-focused coping was added which resulted in variance of about 48.5% (F (3, 48) = 15.1; p< 0.001). Finally, the addition of optimism. To regression model at stage 4 explained variance of 58.2% i.e. additional 9.7% of the variation, and this change in R2 was significant (F (4, 47) = 16.36; p< 0.001). Therefore, it can be inferred that pessimism is the most significant (β = -0.532, p < 0.001) negative determinant of post-traumatic growth among survivors of conflict-related sexual violence. Although all four variables together account for 76% of the variance in PTG, pessimism is the most significant as it explains 25% of the variance.
Table 5
Hierarchal Multiple Regression Analysis to Explore Psychosocial Predictors of Post Traumatic Growth Among Survivors of Conflict-Related Sexual Violence (N=400).
The present study aimed to explore the psychosocial predictors (PTSD, age, gender, coping, locus of control, social support) of PTG for the sample of CRSV survivors from DRC. The result of the present study showed that both positive (PTG=56%) and negative outcomes (PTSD=40%) of CRSV emerged as separate entities and these findings are in line with previous research (Anderson et al., 2019; Johnson et al., 2010; Kelly et al., 2012; Mittelmark et al., 2017; Solomon & Dekel, 2003; Steketee & Foa, 1987; Ullman & Najdowski, 2010). Past studies from various other countries displayed similar findings where survivors of CRSV experienced positive outcomes as well as damaging effects of these experiences (Anderson et al., 2019; Ullman & Najdowski, 2010).
Essentially, optimistically tending people can derive a sense of benefit from adversity; to a greater extent than pessimistic people, and that optimism can be generalized and remains stable over time (Saboonchi et al., 2016). The present study also reported a significant positive value of Pearson correlation for the relationship of PTG with EFC and Optimism. Therefore, it can be inferred that survivors with emotion-focused coping and an optimistic approach toward life have post-traumatic growth, which is also supported by previous literature (Anderson et al., 2019; Solomon & Dekel, 2007). For example, Anderson et al. (2019) reported that if these survivors adopt optimistic ways and have an overall positive approach toward life, they can experience positive psychosocial outcomes in the form of PTG. Additionally, the result of the hierarchal regression model to explore the role of PTSD, pessimism, optimism, and emotion-focused coping in predicting PTG among survivors of CRSV showed that these variables do play a role in predicting PTG. All four variables together account for 76% of the variance in PTG, with pessimism being the most significant as it explains 25% of the variance. The values suggest that pessimism is the most significant (β = -.532, p< 0.000) determinant of PTG among survivors of CRSV. However, PTG is not significantly related to age, social support and problem-focused coping. There are many reasons for it, such as the cognitive makeup of the population. These discoveries are compatible with previous studies (Anderson et al., 2019; Saboonchi et al., 2016; Prati & Pietrantoni, 2009), which reflected that psychosocial, cultural and spiritual capitals are strong buffers in the management of psychological trauma. Along similar lines, a study on survivors of CRSV from Bosnia and Herzegovina showed the same findings where coping strategies played a significant role in the development of PTG (Anderson et al., 2019). The findings of the study prove that pessimism is the most significant predictor of PTG among survivors of CRSV. In addition to pessimism, PTSD, EFC and optimism also play a part in the development of PTG. A recent systematic review conducted by Guggisberg et al. (2021) on 41 articles research articles published between January 2010 and October 2020 focusing on post-traumatic growth following sexual victimization depicted that recovery from sexual victimization is probable with the help of various strategies used by these survivors, such as thoughtful introspection to link with themselves helped them to grow. Therefore, it is important to provide psychological help to cope with pessimism among survivors. Changing their life approach (from pessimism to optimism) and treating the PTSD of survivors of CRSV can be positively effective in their life. Therefore, the survivors of CRSV need to seek psychological help for the development of PTG.
Limitation of Study
While the present study is unique in studying this important issue in Congo, it has some limitations that must be addressed. For example, a small sample limits the generalizability of findings, so future studies with a large and more diverse sample are recommended. Secondly, the use of self-report processes to collect the data is another drawback of the current study, so the study must be replicated by using mix method approach. Thirdly, scales were not available in the local language and were administered with the help of a translator, which is also considered a potential limitation and highlighted the need to adapt these measures in the local context of Congo. The low internal consistency of a few measures might also signify a lack of cross-cultural validity of these measures.
Declaration of patient's consent
The authors certify that informed consent was obtained from all participants using consent forms. The form briefly explains the purpose of the study and ensures that all information will be kept confidential. Furthermore, they were assured they could choose to participate in the study and refuse whenever they wanted. The participants were allowed to ask questions and gave consent once their queries were resolved.
Disclosure statement
The authors have reported no conflict of interest.
References
Ai, A. L., Peterson, C., & Huang, B. (2003). Psychological studies on spiritual and religious development: The case of religion. The International Journal for the Psychology of Religion, 13(1), 29–47. doi.org/10.1207/S15327582IJPR1301_04
Anderson, K., Delić, A., Komproe, I., & et al. (2019). Predictors of post-traumatic growth among conflict-related sexual violence survivors from Bosnia and Herzegovina. Conflict & Health, 13, 23. doi.org/10.1186/s13031-019-0201-5
Carver, C. S. (1997). You want to measure coping, but your protocol is too long: Consider the brief cope. International Journal of Behavioural Medicine, 4(1), 92-100.
Delić, A., Kuwert, P., & Glaesmer, H. (2017). Should the definition of the term 'children born of war' be? Acta Medica Academica, 46(1), 67–69. doi.org/10.5644/ama2006-124.191
Guggisberg, M., Bottino, S., & Doran, C. M. (2021). Women's contexts and circumstances of post-traumatic growth after sexual victimization: A systematic review. Frontier Psychology, doi.org/10.3389/fpsyg.2021. 699288
Jennings, K., & Nikolić-Ristanović, V. (2009). UN Peacekeeping economies and local sex industries: Connections and implications. MICROCON Research Working Paper, 17. Brighton: MICROCON.https://gsdrc.or g/document-library/un-peacekeeping-economies-and-local-sex-industries-connections-and-implications
Johnson, K., Scott, J., Rughita, B., Kisielewski, M., Asher, J., Ong, R., & et al. (2010). Association of sexual violence and human rights violations with physical and mental health in territories of the Eastern Democratic Republic of the Congo. JAMA, 304(5), 553–562. doi.org/10.1001/jama.2010.1086
Jovanović, V., & Gavrilov-Jerković, V. (2013). Dimensionality and validity of the Serbian version of the life orientation test revised in a sample of youths. Journal of Happiness Studies, 14(3), 771–82.
Kelly, J., Kabanga, J., Cragin, W., Alcayna-Stevens, L., Haider, S., & Vanrooyen, M.J. (2012). 'If your husband doesn't humiliate you, other people won't': Gendered attitudes towards sexual violence in the eastern Democratic Republic of Congo. Global Public Health, 7(3), 285–298. https://doi.org/10.1080/17441692.2011.585344
Lazarus, R. S. (1993). Coping theory and research: Past, present, and future. Psychosomatic Medicine, 55, 234–47. doi.org/10.1097/00006842-199 305000-00002
Linden, J. A. (2011). Clinical practice: Care of the adult patient after sexual assault. The New England Journal of Medicine, 365(9), 834–841. doi.org/10.1056/NEJMcp1102869
Macdonald, O. F. (2011). Putting the puzzle together: Factors related to emotional wellbeing in parents of children with autism spectrum disorders. The University of South Florida.
Mittelmark, M. B., & Bauer, G.F. (2017). The meanings of Salutogenesis. The Handbook of Salutogenesis. Springer. https://www.springer.com /gp/book/9783319045993
Najdowski, C. J., & Ullman, S. E. (2009). Prospective effects of sexual victimization on PTSD and problem drinking. Addictive Behaviours, 34(11), 965–968. doi.org/10.1016/j.addbeh.2009.05.004
Prati, G., & Pietrantoni, L. (2009). Optimism, social support, and coping strategies as factors contributing to post-traumatic growth: A meta-analysis. Journal of Loss Trauma. 14(5), 364–88. doi.org/org/10.108 0/15325020902724271
Ruggiero, K. J., Del Ben, K., Scotti, J. R., & Rabalais, A. E. (2003). Psychometric properties of the PTSD Checklist- Civilian Version. Journal of Traumatic Stress, 16, 495-502.
Saboonchi, F., Petersson, L.M., Alexanderson, K., Bränström, R., & Wennman-Larsen, A. (2016). Expecting the best and being prepared for the worst: structure, profiles, and 2-year temporal stability of dispositional optimism in women with breast cancer. Psychooncology, 963, 957–63. doi.org/10.1002/pon.4045
Scheier, M. F., Carver, C.S., & Bridges, M. (1994). Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A re-evaluation of the life orientation test. Journal of Personality and Social Psychology, 67, 1063–78.
Scott, J., Mullen, C., Rouhani, S., & et al. (2017). A qualitative analysis of psychosocial outcomes among women with sexual violence-related pregnancies in the eastern Democratic Republic of Congo. International Journal of Mental Health Systems, 11 (64). doi.org/10.1186/s13033-017-0171-1
Solomon, Z., & Dekel, R. (2007). Post-traumatic stress disorder and post-traumatic growth among Israeli ex-POWs. Journal of Trauma Stress, 20(3), 303–12. https://doi.org/10.1002/jts.20216
Tedeschi, R. G., & Calhoun, L. G. (1996). The post-traumatic growth inventory: Measuring the positive legacy of trauma. Journal of Trauma Stress, 9, 455–71.
Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A., & Keane, T. M. (1993). The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Paper presented at the 9th Annual Conference of the ISTSS, San Antonio, TX.
Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30-41.

