Terrorism inflicts a long-lasting psychological impact on its victims by affecting their overall well-being; however, limited research is available on protection factors. Hence, the present study aimed to explore the predictive role of resilience for psychological distress and well-being among terrorist attack victims. An Interview based quantitative study design was employed. The study sample comprised 200 Participants (men =100, women =100), with an age range between 18 - 60 years old
(M = 30.9, SD = 10.4). Participants included survivors, witnesses, and close family members of the Hazara community living in the terror affected Balochistan province of Pakistan. PCL-5 Checklist, Flourishing Scale and Connor-Davidson Resilience Scale were used to measure the study variables. Findings showed that resilience was negatively correlated with psychological distress and psychological well-being. Moreover, the analyses showed significant gender differences between participants, showing that women scored higher on depression, whereas men scored higher on well-being. The gender difference was found to be insignificant in resilience. Based on the outcomes, it is suggested to include resilience-building initiatives while planning terror victim rehabilitation strategies.
Keywords. Psychological distress, terrorist victims, well-being, resilience
The psychological impact of terrorism on well-being & role of resilience as a moderator
The deleterious effect of Terrorism around the world outstretches beyond the political and economic damage, inflicting psychological distress among its victims. According to worldwide statistics on war and peace, a significant drop in the death toll has been reported (Human Security Report Project, 2013). Despite the significant decrease in wars between countries, acts of terrorism have challenged human security and are enabling dehumanization. Dehumanization explains the mechanism of the impoverishment of human qualities such as honesty, courage, self-awareness, integrity, etc., affecting humans on a personality and spiritual level (Webster, 2016). The rapid cases of terrorism and an intense mode of violence by terrorist groups, brutal and barbaric forms of violence, are spreading fear among citizens across different continents, creating a humanitarian crisis (Waheed, 2018).
Terrorism has a broad impact on culture and disturbs the usual activities of a functioning society by instilling fear among its residents, especially in regions where there is a greater risk of terrorist attacks, such as Pakistan. Between 2003 and December 2017 (South Asia Terrorism Portal, 2017), 22,191 citizens were killed in Pakistan and 6,887 of its rule enforcement administrators due to many terrorist activities. Australia's Institute for Economics and Peace (Global Terrorism Index, 2020) ranks Pakistan seventh in terms of the impact of terrorism. About 867 terrorist attacks have been recorded in Pakistan from 2007 to 2015 on educational institutions, resulting in 392 deaths and 724 injuries (Global Coalition to Protect Education from Attack, 2017). Pakistan is a multicultural and multi-religious country, with 96% of the population. Islam is the dominating religion in Pakistan which is further divided into Sunni-Shia sects. Increasing crime in Pakistan is a direct result of rebellious organizations developing close ties with criminal networks to sustain their activities. Sectarian violence and targeted killings are the new tools of terrorism (Abbasi, 2013).
The Shia Hazara communing, a minority group in Pakistan living in Quetta, Baluchistan Province of Pakistan, has been targeted because of their religious beliefs. Different local armed rebellions combined with sectarian hatred against religious minority groups, such as Shia Hazara Community in Baluchistan (Waheed, 2018), have been targeted by these local insurgents for the past 20 years (Tarar, 2018). Due to their unique facial features, Hazara people are easy to identify; their association with Shia religious sect made them vulnerable to target attacks. According to the National Commission of Human Rights, Hazara Community’s entire population comprises around 0.4 to 0.5 million people. They have been targeted for terrorist attacks since 1999, reporting more than 2,000 deaths in the last 14 years (National Commission of Human Rights, 2018). Besides losing their loved ones, they have faced difficulties pursuing higher education. Furthermore, they have been restricted to a specific area due to fear of persecution. According to NCHR report, Hazaras suffer from several problems, including intense, never-ending violence and limited mobility. This loneliness has led to frustration and despair because being a Hazara seems like a crime.
Psychological sufferings are more prevalent among the victims of terror attacks than physical pain. Most victims appear to have psychological problems, such as PTSD or other similar problems (Gabriel et al., 2007). Different studies have shown the effect of the terrorist attack on the psychological well-being of terrorist victims (Danielsson et al., 2018). However, recent researchers are exploring the role of protective factors in this respect. Resilience is one of the factors that negatively relate to the psychological impacts of terrorism.
The term Resilience refers to the ability to bounce back in the face of challenges. Empirical evidence provides support for the protective role of resilience against mental distress (Kashyap et al., 2014; Singh & Gujral, 2018).
Different aspects of terrorist attacks and the mental health of victims and survivors have been studied earlier; many studies have been carried out to know the effects of terrorism. Most of the research has been carried out in Western countries, and very few have been conducted in non-western societies (Khan et al., 2018; Ramírez et al., 2020; Shah et al., 2018). Most of the available research was focused on survivors of terrorist attacks; however, there is limited research on the family members of victims of terrorist attacks. Most of the families of the victims of terrorism belong to the lower or lower middle class, and many of them have lost their only bread earner of the family. How many incidents affect the families of martyrs also impacts the secondary victims psychologically.
Another point to be highlighted is that each individual responds differently to the traumatic event, depending upon factors such as social context, genetic makeup, past experiences, and expectations for the future (Ursano et al., 1992). Different studies showed different responses to trauma from different genders, such as females reported higher psychological distress than males (Ditlevsen & Elklit, 2010; Haskell, 2010; Irish et al., 2011; Taha & Sijbrandij, 2021). A study (Matud, 2019) shows that males have better well-being overall than females. Also, the presence of resilience within an individual affects the impact of distress on that individual. Thus, this study also highlights the gender differences with respect to the experiences of psychological distress and its effects on their well-being and the presence of resilient skills among its participants.
According to Cuijpers et al. (2009), psychological distress refers to non-specific symptoms of stress, anxiety and depression. Among these issues, post-traumatic stress disorder (PTSD) is a psychological disorder that can occur due to any traumatic experience, such as accidents, natural disasters, terrorist activities, etc., in which the victim may have witnessed death, injury, or any type of physical harm to self or others (Lin et al., 2007; McManus et al., 2007), in response to which victim may manifest symptoms of PTSD. It is a disabling condition that includes nightmares, flashbacks, avoidance and numbing, and hyper-vigilance. According to the APA (2013), out of other mental health-related issues, PTSD is the most frequently occurring disorder after any experience of a traumatic event. Terrorism has influenced the mental health of almost all of its victims, either in the form of PTSD or other related mental health problems (Gabriel et al. 2007). In a study conducted on 1200 veterans, Jordan et al. (1991) estimated that participants currently working in combat forces had PTSD symptoms for about 15%, whereas 30% of the participants developed PTSD throughout life. Also, another study conducted to examine the prevalence and characteristics of post-traumatic stress disorder showed that 28-35% of participants who were directly exposed to terrorist attacks develop PTSD symptoms (Lee et al., 2002).
This current study investigates two aspects of physiological suffering, that is, PTSD and Depressive symptoms. Depression and anxiety are categorized as psychological distress (Mirowsky & Ross, 2002). The research examined the frequency and features of post-traumatic depressive illness in the aftermath of the 9/11 attack and found that nearly 30 % of those subjected to a violent act acquired illness. (Lee et al., 2002), 29% and 31.9% prevalence rate of PTSD was found among females and males, respectively, in a study by Duhok et al. (2021). In a study of Pakistani rescue workers, 15% of participants had clinically relevant PTSD symptoms (Razik et al., 2013).
According to various epidemiological samples, 50% of persons with PTSD are likewise affected by depressive symptoms (Breslau et al., 1997). A study by Kessler et al. (1995) revealed that 48 percent of males and 49 percent of females who faced PTSD had depression too. According to a meta-analysis, around 52% of people with present PTSD also have MDD (Rytwinski et al., 2013). Depression can affect your health and well-being directly and indefinitely. According to research by Flory and Yehuda (2015), the latent structure of PTSD comorbidity shows that people with PTSD who report high negative affectivity and low positive affectivity are more likely to have a comorbid diagnosis of depression
Psychological well-being is a complex construct that concerns optimal psychological functioning and experience. Danier (1984) postulated three distinct features of wellness in one’s life: frequent positive affect, infrequent negative affect, and cognitive evaluations such as life satisfaction. Based on this conceptualization, subjective well-being is measured and assessed as a tripartite construct indexed by (high levels of) life satisfaction and positive affect as well as (low levels of) negative affect (Busseri & Sadava, 2011; Diener, 1984).
A study conducted by Shah et al. (2018) showed that adolescents' psychological well-being was negatively impacted by fear of terrorism. Another study (Khan et al., 2018) found that participants with low psychological well-being levels were likely to have depression. Socio-demographic trends were also significant in this study.
Resilience has been defined by Murphy (1987) as a generic concept concerned with how people cope with stress and how they recover from trauma. It consists of traits such as positive coping, harmony, and compliance. Resilience means adapting and coping with life's calamities and setbacks and not falling apart. Resilience plays a significant role in buffering psychological distress. Different research has studied the protective role of resilience against mental distress. A significant negative association was seen in a study between resilience and depression, stress, and anxiety. A moderated relationship was also observed between COVID-19 and anxiety symptoms with resilience (Traunmüller et al., 2020). In another study, resilience moderated the negative impact of perceived stress on depressive symptoms (da Silva-Sauer, et al., 2021). In a study conducted by Jong-Ku et al. (2016), the role of resilience as a protective factor against PTSD was identified. Their results showed that participants having high self-resilience had lower PTSD symptoms than those with low self-resilience.
Resilience is a personality attribute that vaccinates people from the impact of negative experiences (Connor & Davidson, 2003; Hu et al., 2015). A research study was conducted by Singh and Gujral (2018) to analyze the moderating effect of resilience on role stress and to increase the understanding of how variables like hardiness, internal locus of control, humour, positive outlook, self-efficacy and assertiveness help in developing resilience. The research findings validated the moderating effect of resilience on role stress through critical review and concluded that resilience could be developed over time, and it has a positive outcome in reducing stressors, including role stress. On the other hand, to our knowledge, there is a research gap in exploring the moderating role of resilience for psychological distress and well-being in terrorist victims in Pakistani culture. Hence, the present study focused on addressing this gap in the existing literature.
The rationale of the Study the government has focused and invested a considerable amount of energy and resources in reducing and eliminating terrorist attack incidents while at the same time paying no attention to the victims of such inhumane attacks. Unfortunately, the bereaved families of martyrs are barely remembered, and their sufferings are almost overlooked; they are forgotten entities in our country. This research aims to examine the effect of resilience on the psychological distress and well-being of terror attack victims belonging to the Hazara community. Hazara Community was selected as a sample as it has been constantly targeted by terrorists for the past 20 years (Tarar, 2018), with 2,000 taking allegedly being murdered in the last fourteen years alone (NCHR, 2018). By estimating the impact of psychological distress on the well-being of victims, a proper program for the elimination of psychological distress specifically caused due to PTSD symptoms could be introduced.
Objectives
The objectives of the present research were:
To explore the relationship between psychological distress (i.e., symptoms of PTSD & depression) and the well-being of terrorist attack victims of the Hazara community.
To study moderating effects of resilience between psychological distresses (PTSD & depression) and wellbeing among terrorist attack victims of the Hazara community.
To examine gender differences in the experience of psychological distress, well-being, and resilience among victims of a terrorist attack from the Hazara community.
Method
Sample
This research was conducted on terrorist victims of the Hazara community belonging to one of the affected areas of Pakistan, Baluchistan. The study sample consisted of 200 participants (males = 100 females = 100) having age range between of 18-60 years (M = 30.9, SD = 10.46; 104 participants from 18-30 years, 55 from 31-45 years and 41 participants were in age range of 45-60 years). Victims included survivors, witnesses, and close families of martyrs of the Hazara community were assessed. About 88% of the population had experienced direct threats or injuries during their traumatic experience.
Participants Selection Criteria
Victims of the terrorist attack, which included survivors, witnesses and close families of martyrs of the Hazara community, were assessed. Those who could comprehend the Urdu language were included in the study.
Individuals lesser than age 18 were excluded from the study. Those individuals who have only heard of terrorism but have not experienced the trauma directly or do not fall into either of the prior options were excluded from the study. Those not suffering from any other psychiatric disorder and taking treatment for that per se were also not included.
Instruments
The following instruments were used to assess the participants on the given variables of the study.
Demographic Data Sheet. A demographic data sheet was created, including the respondent's age, gender, education, and questions related to trauma history, e.g., identifying the event, the number of years of exposure to a traumatic event, how the event was experienced and who was the victim.
PTSD Checklist 5 (PCL-5). Urdu-translated PTSD Checklist for DSM-5 (PCL-5; Samsoor et al., 2020) was used to assess psychological distress. It is a 20-item self-report measure that covers 20 signs of PTSD symptoms according to DSM-5. The total symptom severity score is from 0-80. The score ranges from 0-5, where 0 represents a symptom that does not present at all. A total of 10 items from the PCL-5 were evaluated for assessing symptoms of depression and ruling out the possibility of sadness (Questions 9-20). These were Questions 9-20, eliminating questions 10 and 17. Every question was given a rating of four, for a maximum of forty points. The trimmed number for sadness to be considered accepted was set at 50%, resulting in a trimmed value of 20. PCL-5 shows great interior steadiness (Cohen et al., 2015). The authors have reported satisfactory alpha coefficients of the measure.
Flourishing Scale. Urdu version of the Flourishing Scale (Choudhry et al., 2018) was used. This eight-item is a valid and reliable scale that assesses subjective wellbeing among individuals, originally developed by Diener et al. (2009). Scales anchors consist of 7 options, from strongly agree to strongly disagree with the statement. A score between 8 and 56 represents psychological well-being, whereas higher scores in the result show a high level of wellbeing in the respondent. The reliability tests of the flourishing scale confirmed that the values of Cronbach’s alpha coefficient (α = .81) and test-retest (α .82) were acceptable. The Urdu version showed high consistency reliability of alpha coefficient (α = .91).
Connor-Davidson Resilience Scale (CD-RISC-10). The Urdu version of the
Connor-Davidson Resilience Scale (CD-RISC-10) (Connor & Davidson, 1993) was used to test the resilience of the participants. This 10-item scale had scores ranging from 0 - 40, each of which was scored from 0 - 4. The result's highest score shows a higher resilience level in participants. Urdu version scale shows high alpha reliability, i.e., α = .87 (Ghulam et al., 2016).
Procedure
Since the researcher belonged to the specific affected community, he was socially able to approach and negotiate with Hazara Community victims. Written informed consent was acquired from all participants before filling out the questionnaire; afterward, Participants were asked to answer the questions from the questionnaire. Questions were asked of the respondents in a structured interview style. Any participant who was not comfortable with the questions in the questionnaire and wanted to leave the interview even during the administration of the survey was permitted to leave at any point. Members were briefly informed about the objective of the research. The study was approved by the Ethics Committee of the University.
Participants were assured that participation would be retained confidential and the responses would only be used for research purposes. Consent forms were also given to the participants for their willingness for the research purpose. Members were briefly informed about the purpose of the research, the nature of the interview and questionnaire, and its implications. Every respondent that felt uncomfortable with the questionnaire's inquiries and wished to quit the session anywhere at any time was free to do so. The Ethics Committee also approved the study of the University
Results
Data collected in the research were analyzed through the Statistical Package for Social Sciences (SPSS)-25 version. Descriptive statistics of the study variables were calculated. To assess the correlation among study variables, correlational analysis was performed. Linear regressions were used to quantify the significant impacts of the independent factor on the dependent variable. Moderation analysis was also performed.
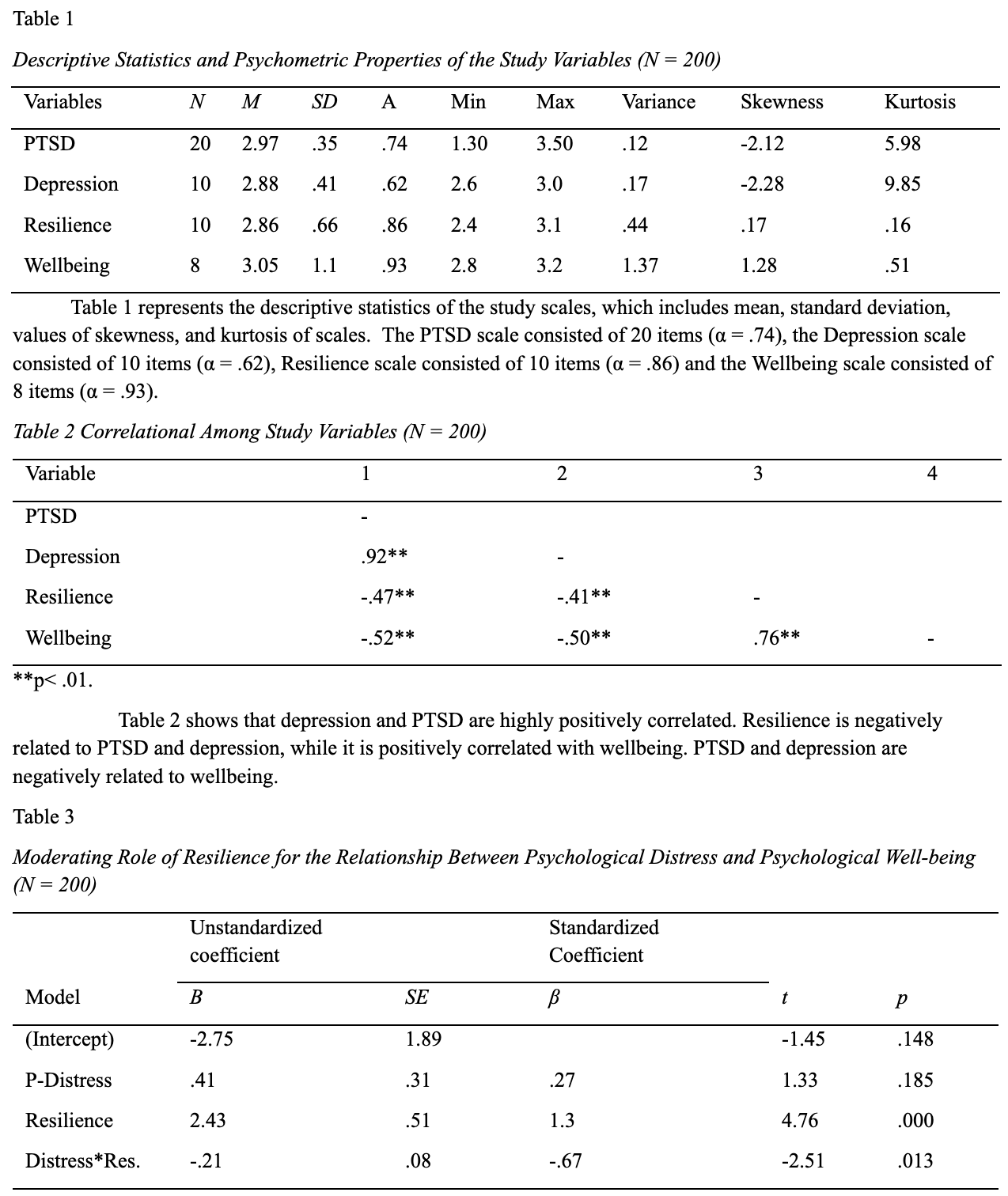
Table 3 shows the moderation effect of resilience between psychological distress and wellbeing. The result reveals that the interaction of resilience and Psychological distress has a positive effect with p-value < 0.05. (R² = 0.636, F (1,199) = 114.1, p < .05).
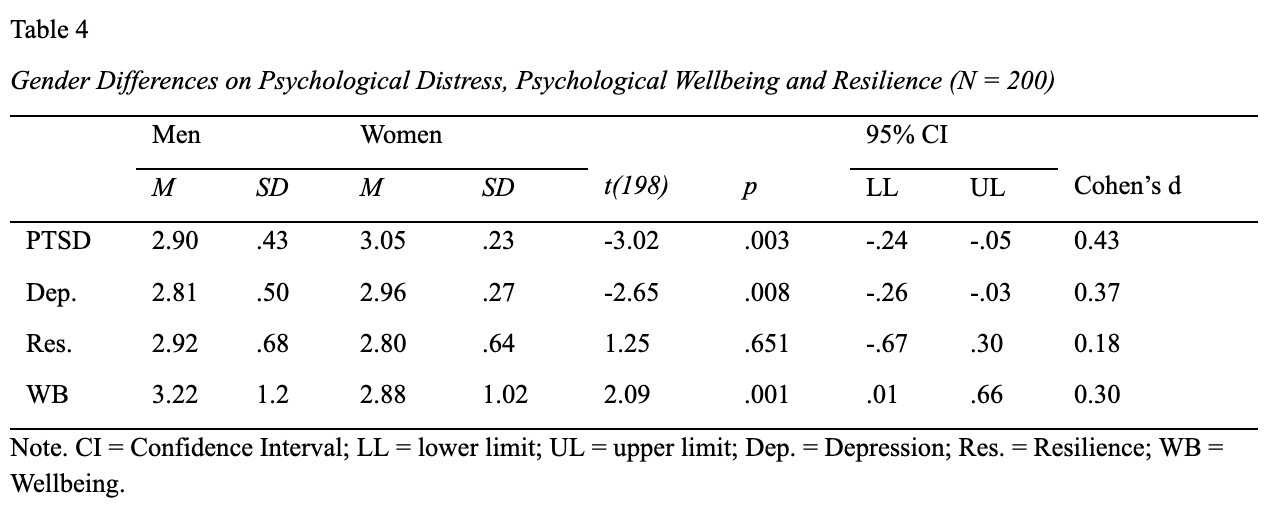
Gender Differences in Psychological Distress (PTSD & Depression), Wellbeing and Resilience
An independent sample t-test was conducted to explore gender differences between men and women.
Table 4 shows significant gender differences in psychological distress (PTSD & depression) and wellbeing. Women report more psychological distress as compared to men, while men score high on psychological well-being. There are no significant gender differences in resilience.
Discussion
The study's main objective was to explore the relationship between psychological distress (i.e., PTSD & depression) and the well-being of terrorist attack victims of the Hazara community. Resilience, having the adaptive ability to cope with stress, trauma, and adversities (Luthar, 2006), has been studied as a moderating factor between psychological distress and well-being.
The prime objective of the study was to examine the relationship between psychological distress and wellbeing among terrorist attack victims. The present study showed a negative association between wellbeing and psychological distress. The main objective of the present research was tested by linear regression analyses, the result of which suggested that psychological distress explained 27% of the variance; and that psychological distress significantly predicts wellbeing among terrorist attack victims.
The findings of our study are consistent with previous studies. For example, a study investigated the impact of distress on the wellbeing of trauma survivors and found a negative correlation between PTSD and wellbeing (Wang et al., 2005). Another study showed that treating symptoms of PTSD and depression significantly improves the overall well-being of an individual (Berle et al., 2018). According to another study, psychological distress, social support, and coping strategies predicted psychological well-being for internally displaced persons (Oginyi et al., 2017).
Objective 1 validated the model of wellness by Danier (1984), that subjective well-being (Andrews & Withey, 1976; Bryant & Veroff, 1982; Diener, 1984). The negative association of psychological distress caused by terrorist attacks with the wellbeing of terrorist attack victims supports the fact that terrorism or terrorist attacks challenge an individual’s existence and safety; this scarcity of safety needs affects the growth of other areas of life (Ryff & Singer, 2008), such as the esteem and self-actualization in individual’s life which consequently impacts the sense of overall wellbeing. The findings of our study are also consistent with the results of the study, which was done to evaluate the effectiveness of treatment programs for PTSD and the comorbid symptoms, which shows significant improvement in the personal wellbeing of clients across the 9-months of the study, indicating that reduced symptoms of psychological distress were associated with improvements in overall personal wellbeing (Berle et al., 2018).
The second objective of the research was to explore the moderating role of resilience in the relationship between psychological distress and wellbeing among terrorist attack victims. The findings of the present research support the moderating role of resilience between psychological distress and wellbeing, suggesting that resilience exerts a strong influence on the impact of psychological distress on the wellbeing of terrorist attack victims. Past literature also showed that resilient people had been found to demonstrate characteristics of effectiveness, high expectancies, positive outlook, self-esteem, internal locus of control, self-discipline, good problem-solving skills, critical thinking skills, and humour (Garmezy, 1991). This notion is supported by the factor model of resilience, which includes personal competence, trust in one's instincts, tolerance of negative affect, strengthening effects of stress, positive acceptance of change, secure relationships, and control (Connor & Davidson, 2003).
Our findings are consistent with past literature. A study conducted by Kashyap et al. (2014) showed that resilience significantly buffered the impact of stress on psychological health. Another study also confirmed the moderation effect of self-efficacy as a component of resilience, which showed that self-efficacy had a direct negative effect on the fear and distress of traumatic events (Mumtaz, 2021). Findings of another research elaborated that a higher level of resilience was associated with lower levels of anxiety and depression symptoms. Additionally, the more resilient individuals recovered from these symptoms after three months, while the less resilient individuals did not show any significant improvement (Leys et al., 2020).
Our last objective was to examine gender differences in psychological distress (PTSD and Depression), wellbeing and resilience in terrorist attack victims. Data were analyzed through a sample t-test. The results of the analyses supported the hypothesis and found significant gender differences in PTSD, Depression, and wellbeing of participants, whereas the gender differences were insignificant in resilience among participants.
Our study is consistent with the findings of the previous studies; Females are at higher risk than males for developing post-traumatic stress disorder symptoms (PTSD) following exposure to trauma (Ditlevsen & Elklit, 2010; Haskell, 2010; Irish et al., 2011; McManus et al., 2007). Taha and Sijbrandij (2021) conducted a cross-sectional survey on 358 female and 464 male adults living in Duhok, Iraq. Their results showed that females reported more somatic and depressive/anxious symptoms than males following a traumatic event. Similarly, results showed that females are more likely to suffer from depression after a traumatic event which is also consistent with previous studies (Harkness et al., 2010; Wang et al., 2019; Young et al., 1990). The present findings also showed significant differences, with the mean score for males being higher than for females. Hence, this confirms that men have better wellbeing overall than women in the current sample, which is consistent with the similar finding where statistically significant differences were found between women and men in some psychological well-being dimensions, with men scoring higher than women (Matud, 2019). The same results have also been found in individualistic countries, such as the United States (Ryff et al., 2006), and in collectivistic countries, such as Japan (Karasawa et al., 2011).
The t-test analysis of gender differences in the resilience of participants in the current study showed no significant differences in the scores for female and male participants. The findings are consistent with the studies where the magnitude of the difference in the means of the level of resilience was found to be very small hence showing no significant gender difference in the resilience of participants (Ebrahimi et al., 2012; Karairmak, 2010). A study conducted on earthquake survivors in Japan also found no difference in resilience levels (as measured by RISC-25) for men and women (Tsuno et al, 2014). Likewise, Liu et al. (2015) also reported insignificant gender differences in levels of resilience in large Chinese community samples. In another study done by Terrill et al. (2016), gender differences in levels of resilience were assessed in a sample with physical disabilities; however, nonsignificant gender differences were found in the sample.
Limitations and Recommendations
For the purpose of an in-depth understanding of the relationship of our variables, participants were chosen from a specific region of Quetta, Baluchistan as incidents of terrorism highly impact it. This prevents the inclusion of other subcultural perspectives or factors from other populations. The study only comprised participants having an age range from 18-60 years; however, individuals below 18, especially children and adolescents, were not included in the study due to the sensitivity of the research and the time constraints in taking parental assent. The research findings being limited cannot provide the difference in levels of the study variables due to development differences displayed by individuals below the age of 18 years. Based on these limitations, it is recommended to collect data from the vast population in terms of age, socio-cultural factors, and region. Furthermore, research needs to be conducted to investigate the specific mechanism by which resilience may help readjustment in individuals after traumatic events; thus, a qualitative account of these experiences may be taken into account in future to further ameliorate the research outcomes.
Study implications
The government has focused and invested a considerable amount of energy and resources in the reduction and elimination of terrorist attack incidents and has not paid sufficient attention to the victims of such attacks. Families of martyrs of terrorist attacks are forgotten entities in our country. As a result of this research paper, we have identified major psychological challenges faced by victims of terrorist attacks. These suggest possible solutions to alleviate psychological discomfort and shift the focus on the help and rehabilitation of terror attack victims. It is recommended that victims' mental health and well-being be considered when formulating policies to address terrorist attacks. Additionally, this research revealed the importance of resilience-building, a tool that supports the general population in dealing with life's challenges. Our findings proposed that psychological distress caused due to the traumatic experience of terrorist attacks affects the wellbeing of victims but constructing resilience among the victims of terrorist attacks population through training experiences may be crucial in ensuring preparedness for high contesting environments and adjustments after such traumatic experiences. Based on the outcomes of the study, it is also recommended to design a resilient building program to strengthen the inner self and be able to process and overcome hardships, specifically in the context of terrorism.
Conclusion
The result of the current study concludes that there is an association between psychological distress and well-being among terrorist attack victims of the Hazara community. A positive correlation was found between PTSD and Depression, while a negative correlation was seen between Psychological Distress (PTSD & Depression) and well-being. Moreover, resilience moderated the relationship between psychological distress and well-being. Resilience reduces the severity of psychological distress. Thus, having strong resilience among terrorist attack victims is considered an important factor in improving their well-being. Having strong attributes that encompass resilience, such as personal competence, trust in one's instincts, tolerance of negative affect, positive acceptance of change, and Control, seem to affect the relationship between psychological distress (PTSD & Depression) caused by terrorist attack incidents and the Wellbeing of victims.
Acknowledgements. The authors would like to thank the victims of the terrorist attacks who participated in the study.
Conflict of interest. None to declare
References
Abbas, S. A., Hassan, A., & Ali, S. (2017). Impact of terrorism on the development of posttraumatic stress disorder (PTSD) among the residents of Khyber Bazaar and its immediately surrounding areas in Peshawar, Khyber Pakhtunkhwa, Pakistan. Pakistan Journal of Pharmaceutical Sciences, 30(1), 205–212. https://pubmed.ncbi.nlm.n ih.gov/28603133/
Abbasi, N. M. (2013). Impact of terrorism on Pakistan. Strategic Studies, 33(2), 33–68. https://www.jstor.org/stable/48527612
Andrews, F. M., & Withey, S. B. (2012). Social indicators of well-being: Americans' perceptions of life quality. Springer Science & Business Media.
Shah, S.A.A., Yezhuang, T., Shah, A.M., Durrani, D. K., & Shah, S.J. (2018). Fear of terror and psychological well-being: The moderating role of emotional intelligence. International Journal of Environmental Research and Public Health, 15(11), 2554. doi.org/10.3390/ijerph151 12554
Berle, D., Hilbrink, D., Russell-Williams, C., Kiely, R., Hardaker, L., Garwood, N., Gilchrist, A., & Steel, Z. (2018). Personal wellbeing in posttraumatic stress disorder (PTSD): association with PTSD symptoms during and following treatment. BMC Psychology, 6(1), 7. doi.org/10.1186/s40359-018-0219-2
Breslau, N., Davis, G. C., Andreski, P., Peterson, E. L., & Schultz, L. R. (1997). Sex differences in posttraumatic stress disorder. Archives of General Psychiatry, 54(11), 1044–1048. doi.org/10.1001/archpsyc.1 997.01830230082012
Bryant, F. B., & Veroff, J. (1982). The structure of psychological well-being: A sociohistorical analysis. Journal of Personality and Social Psychology, 43(4), 653–673. doi.org/10.1037/0022-3514.43.4.653
Busseri, M. A., & Sadava, S. W. (2011). A review of the tripartite structure of subjective well-being: implications for conceptualization, operationalization, analysis, and synthesis. Personality and Social Psychology 15(3), 290-314. doi.org/10.1177/1088868310391271
Choudhry, F.R., Al-Worafi, Y.M., Akram, B., Ahmed, M.A., Anwar Ul Haq, M., Khan, T.M., Rehman, I.U., Barki, N., Munawar, K., Kamal, A., Kassab, Y.W., Bakrin, F.S., Golden, K.J (2018). Factor Structure of Urdu Version of the Flourishing Scale. Frontiers in Psychology, 9, 1513. doi.org/10.3389/fpsyg.2018.01513
Cohen, J., et al. (2015). Preliminary Evaluation of the Psychometric Properties of the PTSD Checklist for DSM – 5. (Conference Presentation). https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
Connor, K. M., & Davidson, J. R. (2003). Developing a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18(2), 76–82. doi.org/10.1002/da.10113
Danielsson, F.B., Larsen, M.S, Nørgaard, B., Lauritsen, J.M. (2018). Quality of life and level of post-traumatic stress disorder among trauma patients: A comparative study between a regional and a university hospital. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 26, 44. doi.org/10.1186/s13049-018-0507-0
Diener, E. (1984). Subjective well-being. Psychological Bulletin, 95(3), 542–575. doi.org/10.1037/0033-2909.95.3.542
Diener, E. et al. (2009) New Measures of Well-Being. https://www.researchgate.net/profile/Robert-BiswasDiener/publicatio n/227284878_New_Measures_of_Well-Being/links/53ece5ce0cf2373 3e80 4d9e9/New-Measures-of-Well-Being.pdf
Ditlevsen, D. N., & Elklit, A. (2010). The combined effect of gender and age on post-traumatic stress disorder: Do men and women show differences in the lifespan distribution of the disorder? Annals of General Psychiatry, 9, 32. doi.org/10.1186/1744-859X-9-32
Ebrahimi, A, Keykhosrovani, M., Dehghani, M., Javdan, M., (2012). Investigating the relationship between a group of undergraduate students' resiliency, spiritual intelligence and mental health. Life Science Journal 9, 67-70. http://www.lifesciencesite.com
Flory, J. D., & Yehuda, R. (2015). Comorbidity between post-traumatic stress disorder and major depressive disorder: alternative explanations and treatment considerations. Dialogues in Clinical Neuroscience, 17(2), 141–150 doi.org/10.31887/DCNS.2015.17.2/jflory
Gabriel, R., Ferrando, L., Cortón, E. S., Mingote, C., García-Camba, E., Liria, A. F., & Galea, S. (2007). Psychopathological consequences after a terrorist attack: an epidemiological study among victims, the general population, and police officers. European Psychiatry: The Journal of the Association of European Psychiatrists, 22(6), 339–346. doi.org/10.1016/j.eurpsy.2006.10.007
Gupta, R. (1998). A Comparative Perspective on the Causes of Terrorism. International Studies, 35(1), 23–53. doi.org/10.1177/0020881798035 001003
Garmezy, N. (1991). Resiliency and Vulnerability to Adverse Developmental Outcomes Associated with Poverty. American Behavioral Scientist, 34(4), 416–430. doi.org/10.1177/00027642910 34004003
Harkness, K. L., Alavi, N., Monroe, S. M., Slavich, G. M., Gotlib, I. H., & Bagby, R. M. (2010). Gender differences in life events prior to the onset of major depressive disorder: the moderating effect of age. Journal of Abnormal Psychology, 119(4), 791–803. doi.org/10.1037/a0020629
Haskell, S. G., Gordon, K. S., Mattocks, K., Duggal, M., Erdos, J., Justice, A., & Brandt, C. A. (2010). Gender differences in rates of depression, PTSD, pain, obesity, and military sexual trauma among Connecticut War Veterans of Iraq and Afghanistan. Journal of Women's Health (2002), 19(2), 267–271. doi.org/10.1089/jwh.2008.1262
Irish, L. A., Fischer, B., Fallon, W., Spoonster, E., Sledjeski, E. M., & Delahanty, D. L. (2011). Gender differences in PTSD symptoms: an exploration of peritraumatic mechanisms. Journal of Anxiety Disorders, 25(2), 209–216. doi.org/10.1016/j.janxdis.2010.09.004
Jordan, B. K., Schlenger, W. E., Hough, R., Kulka, R. A., Weiss, D., Fairbank, J. A., & Marmar, C. R. (1991). Lifetime and current prevalence of specific psychiatric disorders among Vietnam veterans and controls. Archives of general psychiatry, 48(3), 207–215. doi.org/10.1001/archpsyc.1991.01810270019002
Karasawa, M., Curhan, K. B., Markus, H. R., Kitayama, S. S., Love, G. D., Radler, B. T., & Ryff, C. D. (2011). Cultural perspectives on aging and well-being: a comparison of Japan and the United States. International Journal of Aging & Human Development, 73(1), 73–98. doi.org/10.2190/AG.73.1. d
Kashyap, S. P., Kumar, S., & Krishna, A. (2014). Role of resilience as a moderator between the relationship of occupational stress and psychological health. Indian Journal of Health and Wellbeing, 5(9), 1023-1026.
Karairmak, O. (2010). Establishing the psychometric qualities of the Connor Davidson Resilience Scale (CD-RISC) using exploratory and confirmatory factor analysis in a trauma survivor sample. Psychiatry Research. 179, 350-356. doi.org/10.1016/j.psychres.2009.09.012
Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52(12), 1048–1060. https://doi.org/10.1001/archpsyc.1995.03950240066012
Khan, A., Ullah, O., Nawaz, K., Arsalan, Ambreen, & Ahmad, I. (2018). Post-traumatic stress disorder among school children of Army Public School Peshawar after Six months of a terrorist attack. Pakistan journal of medical sciences, 34(3), 525–529. doi.org/10.12669/pjms.343.14 885
Lee, A., Isaac, M., & Janca A. (2002). Post-traumatic stress disorder and terrorism. Current Opinion in Psychiatry 15(6):633–7. doi.org/10.1097/00001504-200211000-00013
Lee, J. K., Choi, H. G., Kim, J. Y., Nam, J., Kang, H. T., Koh, S. B., & Oh, S. S. (2016). Self-resilience as a protective factor against the development of post-traumatic stress disorder symptoms in police officers. Annals of occupational and environmental medicine, 28, 58. doi.org/10.1186/s40557-016-0145-9
Leys, C., Kotsou, I., Shankland, R., Firmin, M., Péneau, S., & Fossion, P. (2021). Resilience Predicts Lower Anxiety and Depression and Greater Recovery after a Vicarious Trauma. International Journal of Environmental Research and Public Health, 18(23), 12608. doi.org/10.3390/ijerph182312608
Liu, D., Schmidt, A. F., Burns, R., & Roberts, R. (2015). The Connor Davidson Resilience Scale: establishing invariance between gender across the lifespan in a large community-based study. Journal of Psychopathology and Behavioral Assessment, 340-348. doi.org/10.1007/s10862-014-9452-z
Luthar, S. S. (2006). Resilience in development: A synthesis of research across five decades. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology: Risk, disorder, and adaptation (pp. 739–795). John Wiley & Sons, Inc. https://psycnet.apa.org/record/2 006-03609-020
Matud, M. P., López-Curbelo, M., & Fortes, D. (2019). Gender and Psychological Well-Being. International Journal of Environmental Research and Public Health, 16(19), 3531. doi.org/10.3390/ijerp h16193531
Mcmanus, S., Seville, E., Brunsdon, D., & Vargo, J. (2007). Resilience management: A framework for assessing and improving the resilience of organizations. Resilient Organizations Research Report https://ir.canterbury.ac.nz/handle/10092/2808
Mirowsky, J., & Ross, C. E. (2002). Measurement for human science. Journal of health and social behavior, 43(2), 152–170.
Mumtaz, A., Manzoor, F., Jiang, S., & Rahaman, A.M. (2021). COVID-19 and Mental Health: A Study of Stress, Resilience, and Depression among the Older Population in Pakistan. Healthcare. 9, 424. doi.org/10.3390/healthcare9040424
Oginyi, R. C. N., et al. (2016). Depression, Psychological Distress, Social Support and Coping Strategies as Predictors of Psychological Well-Being Among Internally Displaced Persons. Middle-East Journal of Scientific Research 25(6), 1269-1279. doi.org/10.5829/idosi.mejs r.2017.1269.1279
Razik, S., Ehring, T., & Emmelkamp, P. M. (2013). Psychological consequences of terrorist attacks: prevalence and predictors of mental health problems in Pakistani emergency responders. Psychiatry Research, 207(1-2), 80–85. doi.org/10.1016/j.psychres.2012.09.031
Ryff, C. D., Love, G. D., Urry, H. L., Muller, D., Rosenkranz, M. A., Friedman, E. M.,et al. (2006). Psychological well-being and ill-being: Do they have distinct or mirrored biological correlates? Psychotherepy & Psychosomatic 75, 85–95. doi.org/10.1159/000090892
Ryff, C. D., & Singer, B. H. (2008). Know thyself and become what you are: A eudaimonic approach to psychological well-being. Journal of Happiness Studies: An Interdisciplinary Forum on Subjective Well-Being, 9(1), 13–39. doi.org/10.1007/s10902-006-9019-0
Rytwinski, N. K., Scur, M. D., Feeny, N. C., & Youngstrom, E. A. (2013). The co-occurrence of major depressive disorder among individuals with posttraumatic stress disorder: a meta-analysis. Journal of Traumatic Stress, 26(3), 299–309. doi.org/10.1002/jts.21814
Taha, P. H., & Sijbrandij, M. (2021). Gender Differences in Traumatic Experiences, PTSD, and Relevant Symptoms among the Iraqi Internally Displaced Persons. International Journal of Environmental Research and Public Health, 18(18), 9779. doi.org/10.3390/ijerp h18189779
Tarar, A. U. (2018, November 12). Targeted killing of Hazaras. DAWN.COM. https://www.dawn.com/news/1445093
Tsuno, K., Oshima, K., Kubota, K., & Kawakami, N. (2014). Personal resilience and post-traumatic stress symptoms of local government employees: six months after the 2011 magnitude 9.0 East Japan Earthquake. Journal of Occupational Health, 56(6), 245–258.doi.org/10.1539/sangyoeisei.B14006
Waheed, A. (2018). Victims of terrorism in Pakistan: Review of existing victim services and scope of improvement. Wolf Publishers. https://research.tilburguniversity.edu/en/publications/victims-of-terrorism-in-pakistan-%09review-of-existing-victim-servic
Wang, C. H., Tsay, S. L., & Bond, A. E. (2005). Post-traumatic stress disorder, depression, anxiety and quality of life in patients with traffic-related injuries. Journal of Advanced Nursing, 52(1), 22–30. doi.org/10.1111/j.1365-2648.2005.03560.x
Wang, P., Li, B., Fan, J., Zhang, K., Yang, W., Ren, B., & Cui, R. (2019). Additive antidepressant-like effects of fasting with β-estradiol in mice. Journal of Cellular and Molecular Medicine, 23(8), 5508–5517. doi.org/10.1111/jcmm.14434
Young, M. A., Fogg, L. F., Scheftner, W. A., Keller, M. B., & Fawcett, J. A. (1990). Sex differences in the lifetime prevalence of depression: does varying the diagnostic criteria reduce the female/male ratio? Journal of Affective Disorders, 18(3), 187–192. https://doi.org/10.1016/0165-0327(90)90035-7

